

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Following the first report of 2009 pandemic influenza A (H1N1; hereafter referred to H1N1 2009) in April 2009, the infection became a pandemic. The drugs of choice for the treatment and prophylaxis of H1N1 2009 are neuraminidase inhibitors including oseltamivir (Tamiflu® [Roche]) and zanamivir (Relenza® [GlaxoSmithKline]). However, increasing use of oseltamivir has led to the emergence of the oseltamivir-resistant H1N1 2009 virus, which harbors an H274/275Y or I223V neuraminidase mutation. As of 9 February 2011, 370 cases of oseltamivir-resistant H1N1 2009 infection had been reported to the World Health Organization.1
It has been suggested that oseltamivir-resistant seasonal influenza or H1N1 2009 harboring the H274/275Y mutation is less virulent than are strains that are oseltamivir-sensitive.2-4 For this reason, fatal infections by these resistant viruses are rarely reported,5-7 although fatalities have occurred in severely immunocompromised patients with hematologic disorders or cancer with prolonged viral shedding despite oseltamivir therapy. Some adult cases of oseltamivir-resistant H1N1 2009 have also been reported in Korea; however, these were not fatal despite the presence of prolonged viral shedding.8,9
Here, we report a rapidly fatal case of oseltamivir-resistant H1N1 2009 in an adult patient in Korea.
CASE REPORT
A 60-year-old male Korean visited Chonnam National University Hospital because of chest pain and shortness of breath for 7 days. The patient had hypertension and diabetes mellitus as underlying diseases, which had been diagnosed 15 years previously. The patient had end-stage renal disease and had been receiving hemodialysis for 2 years. The patient also had dilated cardiomyopathy; his cardiac ejection fraction was 36% with global hypokinesia, and the end-diastolic and end-systolic diameters of the left ventricle were 65 mm and 54 mm, respectively, on echocardiography. The patient began empiric therapy with oseltamivir (75 mg twice per day) within 24 h of the development of symptoms, which was prescribed at a local clinic. However, his symptoms were not relieved.
Upon admission to our institution, the patient had respiratory symptoms of coughing and blood-tinged sputum. No febrile sense was evident. Other examination findings were a blood pressure of 120/80 mmHg, pulse rate of 63 beats/min, respiratory rate of 20/min, and body temperature of 36℃. Crackle was present in both lower lung fields on chest auscultation.
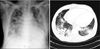
The initial laboratory examination revealed a white blood cell count of 15,400/mm3, a hemoglobin level of 10.1 g/dl, and a platelet count of 141,000/mm3. His C-reactive protein level was 8.6 mg/dl. On initial arterial blood analysis, the values of pH, PaO2, PaCO2, and bicarbonate ions were 7.365, 49.0 mmHg, 33.3 mmHg, and 18.6 mmol/L, respectively. Cardiomegaly and pulmonary infiltration in the right lower, right middle, and left lower lobes were observed on chest radiography and computed tomography (Fig. 1). The Acute Physiology and Chronic Health Evaluation (APACHE) II score and pneumonia severity index of the patient upon presentation were 26 and 151, respectively. Urinary antigen tests for Streptococcus pneumoniae and Legionella were negative.
After blood and sputum sampling for respiratory virus analysis, reverse-transcriptase polymerase chain reaction (RT-PCR) and bacterial culture, empirical intravenous antibiotic therapy with ceftriaxone and clindamycin was initiated. On the second day of hospitalization, the patient was intubated and mechanical ventilation was started because of clinical deterioration. Sputum RT-PCR for H1N1 2009 was performed on hospital days one and three. On the fourth day of hospitalization, sputum RT-PCR for H1N1 2009 from a specimen acquired on hospital day three was positive. Bacterial sputum and blood cultures were negative. The APACHE II score and pneumonia severity index of the patient were aggravated to 37 and 191, respectively. The patient was isolated and began to receive a double dose of oseltamivir therapy (150 mg twice per day). The initial antibiotics were changed to ceftriaxone and levofloxacin. Despite administration of oseltamivir and antibiotics, mechanical ventilation, inotropics, and continuous renal replacement therapy, the patient's pneumonia worsened and led to multi-organ failure. The patient died on the sixth day of hospitalization, despite 3 days of antiviral therapy and 6 days of antibacterial therapy. Sequence analysis performed at the Korea Centers for Disease Control and Prevention revealed an H275Y neuraminidase gene mutation, as described elsewhere.10
DISCUSSION
We have presented the case of a 60-year-old Korean male patient who was infected with oseltamivir-resistant H1N1 2009, which proved lethal. Oseltamivir-resistant H1N1 2009 was first reported in September 2009, and the number of cases has been steadily increasing, including in South Korea.1,10 Although the incidence of oseltamivir-resistant H1N1 2009 infections is increasing, fatal cases have been reported only rarely. In South Korea, the present case is the first fatal one in an adult.
The present case shows some differences in clinical characteristics compared to previously reported fatal cases. First, unlike our case, most fatal cases of oseltamivir-resistant virus infection have occurred in patients with severe immunosuppression associated with hematologic disorders or cancer.5-7 Second, the clinical course of oseltamivir-resistant virus infection is usually insidious despite inappropriate antiviral therapy, because the virulence of oseltamivir-resistant influenza virus is thought to be lower than that of oseltamivir-sensitive viruses.8,9 Animal studies have suggested that oseltamivir-resistant H1N1 2009, as well as seasonal influenza, is less virulent and less transmissible than oseltamivir-sensitive viruses. In the present case, however, although the infection was caused by oseltamivir-resistant virus, pneumonia progressed rapidly and led to death. This suggests that some clone of oseltamivir-resistant H1N1 2009 is sufficiently virulent to cause rapidly fatal pneumonia. Third, most cases of oseltamivir-resistant virus infections have occurred in patients who had undergone prolonged oseltamivir therapy.5-9 The present patient was treated short-term with oseltamivir before acquisition of oseltamivir resistance. This highlights that oseltamivir resistance after short-term drug exposure is also possible, and that the use of zanamivir should be considered in patients with clinical deterioration, despite oseltamivir therapy.
 XML Download
XML Download