

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In recent studies, drug-eluting stents (DES) were more widely used than bare-metal stents (BMS) in patients who underwent percutaneous coronary intervention (PCI).1 Recently, several significant complications after implantation of DES have been reported, and stent thrombosis (ST) is a rare but fatal complication among them. Discontinuation of dual antiplatelet therapy is known to be a risk factor for ST in patients after implantation of DES.2-4 Therefore, dual antiplatelet therapy is recommended to be maintained for at least 12 months after stent implantation to prevent late stent thrombosis (LST) or very late stent thrombosis (VLST). However, it is still unclear how long dual antiplatelet therapy is needed and when the antiplatelet therapy can be safely stopped.
Here we report a case of a patient with acute myocardial infarction due to VLST that occurred 1 week after discontinuation of 5 years of dual antiplatelet therapy after implantation of a sirolimus-eluting stent.
CASE REPORT
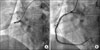
A man with no risk factors for coronary artery disease except smoking underwent PCI in May 2005 at age 44. A 3.0×23 mm Cypher® stent was deployed in the proximal right coronary artery. The patient was placed on aspirin and clopidogrel as antiplatelet therapy. He experienced no adverse events. Five years later, the patient was advised to stop taking clopidogrel. Seven days after the discontinuation of clopidogrel, he experienced severe chest pain and was transported to the emergency room by ambulance. A physical examination revealed a temperature of 36.0℃, blood pressure of 90/60 mmHg, and a regular heart rate of 100 beats/min without murmur or gallop. Pulmonary rales, peripheral edema, or other clinical signs of congestive heart failure were not present. An electrocardiogram revealed ST-segment elevation in lead II, III, and aVF. The peak level of creatine kinase (CK) was 1,334 U/L, CK-MB was 75.4 U/L, and troponin-I was 38.1 ng/ml. Transthoracic echocardiography in the emergency room revealed inferior wall akinesia, and his ejection fraction was 45%. The patient received 300 mg of aspirin and 600 mg of clopidogrel as a loading dose and was transferred to the cardiac catheterization laboratory. His pain to door time was about 60 minutes, and the door to balloon time was 72 minutes. An emergent coronary angiogram revealed a thrombotic total occlusion at the proximal right coronary artery (Fig. 1A). The occluded right coronary artery was revascularized successfully by balloon angioplasty with a 3.0×20 mm balloon (Fig. 1B). After PCI, Ultegra Rapid Platelet Function Assay (RPFA)-ASA and Ultegra RPFA-P2Y12 (VerifyNow™Assay) were performed to determine aspirin and clopidogrel resistance. Aspirin resistance was defined as an aspirin reaction unit (ARU) ≥550. Clopidogrel resistance was defined as percent inhibition of P2Y12 less than 20%. The patient's ARU was 350 and his P2Y12 was 70%.
The patient was discharged uneventfully and followed up with dual antiplatelet therapy of aspirin and clopidogrel. There have been no adverse events with clinical follow-up for 1 year, and a follow-up coronary angiogram revealed no significant stent restenosis.
DISCUSSION
DES interrupt re-endothelialization of the vessels, which results in a lower rate of target lesion revascularization than with BMS. However, delayed vascular healing after PCI may cause ST. Premature discontinuation of antiplatelet therapy is the most common precipitating factor of ST. Long and multiple stents, stent under-expansion or stent malposition, residual dissection, and resistance to aspirin and clopidogrel have been suggested as other possible causes of ST.5-7 Several studies revealed a higher rate of LST and VLST after DES implantation than after BMS implantation. Dual antiplatelet therapy reduces subacute thrombotic events after PCI, and at least 12 months of dual antiplatelet therapy after PCI is recommended in the current guidelines to prevent ST.
However, the duration of dual antiplatelet therapy is not precisely defined. Whether long-term maintenance of dual antiplatelet therapy can prevent LST or VLST is still controversial. Park et al reported that clopidogrel continuation beyond 1 year did not appear to decrease stent thrombosis and clinical events after DES implantation,8 although Tanzili et al concluded that 2 years of dual antiplatelet therapy can prevent the occurrence of VLST after DES implantation.9
Triple antiplatelet therapy adding cilostazol is considered to be another choice for preventing stent thrombosis in patients with clopidogrel resistance or for the prevention of recurrent stent thrombosis. The disadvantage of triple therapy is the bleeding tendency, but the bleeding tendency of triple therapy was reported to be not much higher than that of dual antiplatelet therapy in several studies. However, the effect of triple therapy on long-term survival or cardiac events is controversial as well.10,11
In this patient, there were no risk factors for ST except former smoking and no evidence of aspirin or clopidogrel resistance. The patient had been treated with dual antiplatelet agents for enough time (5 years) after DES implantation, but VLST occurred at 1 week after discontinuation of clopidogrel.
We concluded that 12 months of dual antiplatelet therapy may not be enough for the prevention of LST or VLST after DES implantation in some patients who do not show complete re-endothelialization of the coronary artery. Concerning the decision to cease clopidogrel therapy, we suggest that it should depend on the condition of the patient and risk factors for ST such as underlying disease, the length or location of the lesion, the resistance of aspirin or clopidogrel, and so on. It seems difficult to decide when the dual antiplatelet therapy can be safely stopped. Perhaps the development of imaging systems such as optical coherence tomography will give us more precise information. We suggest that physicians educate their patients about the hazards of premature cessation of dual antiplatelet therapy and delay performing surgical procedures until 1 year after implantation of DES. Further studies are required to prevent LST or VLST after implantation of DES.
 XML Download
XML Download