

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Arteriovenous malformation (AVM) of gastrointestinal tract is uncommon, especially tumorous or polypoid AVM is very rare. Polypoid AVMs usually appear pedunculated or semipedunculated solitary mass and can be treated by conventional polypectomy or endoscopic mucosal resection [1]. To the best of our knowledge, seventeen cases of polypoid intestinal AVMs have been reported in the English-language literature and only three cases were located in jejunum [12]. In the series of 17 cases, the size of polypoid AVMs was ranged from 0.4 to 8 cm.
However, we experienced a 13.5-cm-sized AVM which compressed the intestinal lumen and caused intestinal obstruction. We believed it remained asymptomatic for a long time because it was an outbulging mass from submucosa to subserosa instead of intraluminal growth. As far as we know, such a huge outbulging AVM mass has not been reported. We here report an unusual giant jejunal AVM, which is mimicking a subepithelial intestinal tumor.
CASE REPORT
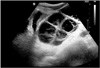
A 15-year-old boy presented at the emergency room with several episodes of nausea, vomiting, intense abdominal pain and distension. The abdominal pain was developed 7 days ago and aggravated on admission day. On initial physical examination, abdominal ileus was suspected. He did not complain of any signs of gastrointestinal bleeding, such as melena or hematochezia. His body temperature was 37.1℃ and laboratory tests including complete blood counts, liver and renal function were within normal range. Ultrasonography and contrast-enhanced CT revealed an about 13 cm sized multiseptated cystic mass in pelvic cavity (Fig. 1). The mass was entirely cystic appearance without any enhancing solid portion. The cystic lumen showed echogenic internal hemorrhage on ultrasonography. The overlying small intestine was diffusely dilated. On operation, a huge cystic mass was palpated in the jejunum about 15 cm below from the ligament of Treiz. He underwent segmental resection and primary anastomosis, under the diagnosis of intestinal obstruction by small bowel tumor. On gross examination of the specimen, the mucosa was intact but slightly hyperemic and a well demarcated submucosal outbulging mass measuring 13.5×7.0×5.5 cm was noted. The external surface of mass was multilobulated and congested. On section, the mass was multilocular cystic appearance separated by fibrous septa and contained bloody materials (Fig. 2A). Histopathologic evaluation demonstrated variable sized large, twisted or thick walled vessels characterized by arteries and veins without intervening capillaries, which were observed in the submucosa extending into subserosa (Fig. 2B). Some veins were markedly dilated and ruptured. This finding was consistent with AVM with phlebectasia. There was no solid tumor-like portion. After operation, he is healthy without any complication.
DISCUSSION
AVM is an abnormal connection between arteries and veins, bypassing the capillary system. This vascular anomaly is generally occurred in the central nervous system, but possibly appeared in any other organs. AVM of the gastrointestinal tract is uncommon. Although most of AVMs are asymptomatic, they may manifest with intense abdominal pain or bleeding. AVM of the gastrointestinal tract could be occurred at any age. Intestinal AVMs usually involve cecum and right side colon in adult [123]. However, AVMs of children are frequently developed in jejunum and result in obstruction or intussusception [45]. The present case of jejunal AVM in 15-year-old boy is accordant to that.
Typical endoscopic finding of colonic AVM reveals bright red and flat mucosal lesion with irregular border. According to Yano-Yamamoto's endoscopic classification of small intestinal vascular lesions, AVMs usually appear as pulsatile red protrusion with surrounding venous dilatation [6]. Intestinal AVM that appears as mass or polypoid lesion is extremely rare as like our case. Most reported polypoid AVMs were pedunculated or semipedunculated type overlaid by hyperemic mucosa. The largest size of AVM was 8.5 cm in longest diameter located in sigmoid colon in a 68-year-old man and removed by endoscopic resection [7]. Our case of AVM demonstrates the largest size that has ever been reported before. And, this AVM lesion was observed in submucosa extending to subserosal layer, which formed a huge outbulging tumor-like lesion. Some veins were abnormally dilated and ruptured spontaneously. Sometimes AVMs may result in life-threatening hemorrhage. However, in our case, the mucosa showed no exposed blood vessel, so the patient did not complain gastrointestinal bleeding despite of huge mass size.
Moore et al. [8] classified vascular lesions of gastrointestinal tract into three types based on patient's age, location, macroscopic appearance, and family history. Type 1 lesions usually occurred in patients over 55 years, which were small solitary lesions and typically affect the right colon. These lesions are thought to be acquired and are commonly referred to as angiodysplasia or vascular ectasia. Type 2 lesions occurred in patients younger than 55 years and were much larger size, usually in the small bowel. These lesions are thought to be congenital. Type 3 lesions were punctate angiomas causing gastrointestinal hemorrhage. These include hereditary hemorrhagic telangiectasia and are associated with respiratory and cutaneous lesions. According to this classification, our case is close to type 2 lesion. However, Moore et al. [8] evaluated very limited cases because the rarity of intestinal AVMs. If possible, further large scaled study is expected.
As the differential diagnosis, angiodysplasia and Dieulafoy's lesion must be considered. Pathologically, AVM is distinct from angiodysplasia or Dieulafoy's lesion. AVM appears as tangles of various sized abnormal vessels that have characteristics of arteries and veins without capillary beds. But angiodysplasia is characterized by venous or capillary distension. Dieulafoy's lesion is characterized by an abnormal, submucosal, caliber-persistent artery that typically protrudes through a minute mucosal defect [6].
Because there have been a few case reports of synchronous development of gastrointestinal stromal tumor (GIST) and AVM, we thoroughly examined the mass especially the thick-walled portion to exclude the co-existence of GIST [910]. But any component of GIST was not found in this case. Immunohistochemistry for CD34 and KIT were also negative.
Although intestinal tumorous or polypoid AVM is extremely rare, it should be considered in young patient with intestinal obstruction or bleeding. The diagnosis of AVM can be made based on endoscopic finding, angiography or CT scan. However it might be misdiagnosed as subepithelial intestinal tumor or GIST. We report an unusual giant jejunal AVM, which cause intestinal obstruction in 15-year-old boy.

 XML Download
XML Download