

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
Minimally invasive surgery (MIS) in abdomen and thorax has been widely accepted for pediatric diseases. Thoracoscopic surgery has the advantage of less pain, better cosmetic outcomes and less musculoskeletal sequelae in comparison to open surgery. We would like to share our initial experience with thoracoscopic surgery performed by one pediatric surgeon.
Methods
We performed a retrospective review of patients who underwent thoracoscopic surgery by one pediatric surgeon between April 2010 and August 2017 in Department of Pediatric Surgery, Seoul National University Children's Hospital.
Results
There were totally 18 cases; 8 cases for esophageal atresia, 3 cases for congenital diaphragm hernia, 2 cases for diaphragm eventration, 2 cases for esophageal duplication cyst, 2 cases for pleural mass and 1 case for esophageal bronchus. At the operation, median age was 9.5 months (range, 0-259 months) and median body weight was 9.4 kg (range, 1.9-49.4 kg). Median operative time was 157.5 minutes (range, 45-335 minutes). There was no case of open conversion and 2 cases of minor leakage at anastomosis site in case of esophageal atresia. Median follow-up month was 5 months (range, 0-87 months). During follow-up, 4 cases of esophageal atresia showed anastomosis site narrowing and average 2.5 times (range, 1-5 times) of esophageal balloon dilatation was done.
Figures and Tables
Fig. 1
Esophageal atresia (EA) with tracheoesophageal fistula. (A) Position of patient for operation of EA (white dots, working port; black dot, camera port). (B) After ligating azygos vein, fistula was also ligated with simple suture, and end-to-end anastomosis of esophagus was done with interrupted suture. Arrow, end-to-end anastomosis site.

Fig. 2
Esophageal atresia, Gross type A. (A) After 7 months, he underwent thoracoscopy and laparoscopy surgery simultaneously by gastric tube interposition. (B) Stomach was incised along great curvature with endo GIA, and gastric tube was made. (C) Gastric tube with distal esophagus was interpositioned to thorax, and esophagoesophagostomy was done by thoracoscopy. Arrows: a, gastric tube-distal part of esophagus; b, proximal part of esophagus. Arrowheads, resected with Endo GIA (Covidien, USA).

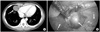
Fig. 3
Esophageal duplication cyst located at posterior mediastinum. (A) The mass was abutting with anterior wall of esophagus on chest CT (2.5×1.9×2.5-cm-sized mass). (B) Mass was connected to muscle layer of esophagus. Arrows: a, mass; b, esophagus.

Fig. 4
Esophageal duplication cyst of superior mediastinum. (A) There was a mass situated at just front of upper esophagus on neck MRI (2.5×2.2×4.5-cm-sized mass). (B) There was a mass at the front and right of the esophagus. Arrows: a, esophageal duplication cyst; b, true esophagus.

Fig. 5
Esophageal bronchus. (A) Upper gastrointestinal series showed a community between esophagus and trachea. The contrast also showed that bronchus and bronchioles are risen from esophagus. (B) Intraoperative photo. There was fistula tract between bronchus and esophagus, so it was ligated with simple suture. Patient underwent thoracoscopic right upper lobectomy and fistula division. Arrows: a, fistula tract; b, esophagus.

Fig. 6
Congenital diaphragm hernia. (A) There was hernia sac on right diaphragmatic defect. (B) Hernia sac was excised and primary repair was performed. Arrows: a, hernia sac; b, primary closure.

Fig. 7
Venous malformation. (A) There was mass at cardoiphrenic angle and it was suspected an inflammatory pseudo-tumor or congenital lung lesion like cystic lymphangioma on chest CT (3.0×3.6×2.3-cm-sized mass). (B) It was being originated from right pleura and was resected clearly. Arrows: a, mass; b, lung; c, diaphragm.

References
1. Wall JK, Sinclair TJ, Kethman W, Williams C, Albanese C, Sylvester KG, et al. Advanced minimal access surgery in infants weighing less than 3kg: a single center experience. J Pediatr Surg. 2017; 05. 11. [Epub ahead of print]. DOI: 10.1016/j.jpedsurg.2017.05.006.
2. Lieber J, Urla CI, Baden W, Schäfer J, Kirschner HJ, Fuchs J. Experiences and challenges of thorcoscopic lung surgery in the pediatric age group. Int J Surg. 2015; 23:169–175.
3. Holcomb GW 3rd. Thoracoscopic surgery for esophageal atresia. Pediatr Surg Int. 2017; 33:475–481.
4. Yang YF, Dong R, Zheng C, Jin Z, Chen G, Huang YL, et al. Outcomes of thoracoscopy versus thoracotomy for esophageal atresia with tracheoesophageal fistula repair: a PRISMA-compliant systematic review and meta-analysis. Medicine (Baltimore). 2016; 95:e4428.
5. Huang JS, Lau CT, Wong WY, Tao Q, Wong KK, Tam PK. Thoracoscopic repair of congenital diaphragmatic hernia: two centres' experience with 60 patients. Pediatr Surg Int. 2015; 31:191–195.
6. Bax KMA, Georgeson KE, Rotehenberg SS, Valla JS, Yeung CK. Endoscopic surgery in infants and children. Berlin: Springer;2008.
7. Seo JM. Pediatric minimal invasive surgery. J Korean Assoc Pediatr Surg. 2011; 17:111–124.
8. Zani A, Lamas-Pinheiro R, Paraboschi I, King SK, Wolinska J, Zani-Ruttenstock E, et al. Intraoperative acidosis and hypercapnia during thoracoscopic repair of congenital diaphragmatic hernia and esophageal atresia/tracheoesophageal fistula. Paediatr Anaesth. 2017; 27:841–848.
9. Tytgat SH, van Herwaarden MY, Stolwijk LJ, Keunen K, Benders MJ, de Graaff JC, et al. Neonatal brain oxygenation during thoracoscopic correction of esophageal atresia. Surg Endosc. 2016; 30:2811–2817.
10. Kim D. Current status of pediatric Minimal Invasive Surgery (MIS) in Korea. J Minim Invasive Surg. 2016; 19:84–88.
11. Holcomb GW 3rd, Rothenberg SS, Bax KM, Martinez-Ferro M, Albanese CT, Ostlie DJ, et al. Thoracoscopic repair of esophageal atresia and tracheoesophageal fistula: a multi-institutional analysis. Ann Surg. 2005; 242:422–428. discussion 428-30.
12. St Peter SD, Ostlie DJ. Laparoscopic gastric transposition with cervical esophagogastric anastomosis for long gap pure esophageal atresia. J Laparoendosc Adv Surg Tech A. 2010; 20:103–106.
13. Sethi GK, Marsden J, Johnson D. Duplication cysts of the esophagus. South Med J. 1974; 67:616–618.
14. Bratu I, Laberge JM, Flageole H, Bouchard S. Foregut duplications: is there an advantage to thoracoscopic resection? J Pediatr Surg. 2005; 40:138–141.
15. Fujishiro J, Ishimaru T, Sugiyama M, Arai M, Suzuki K, Kawashima H, et al. Minimally invasive surgery for diaphragmatic diseases in neonates and infants. Surg Today. 2016; 46:757–763.
16. Becmeur F, Reinberg O, Dimitriu C, Moog R, Philippe P. Thoracoscopic repair of congenital diaphragmatic hernia in children. Semin Pediatr Surg. 2007; 16:238–244.
17. Li B, Chen BW, Wang QS, Wang BY. Thoracoscopic repair of diaphragmatic hernia in infants: a new modification of the technique. Eur J Pediatr Surg. 2016; 26:519–523.
18. Clark RH, Hardin WD Jr, Hirschl RB, Jaksic T, Lally KP, Langham MR Jr, et al. Current surgical management of congenital diaphragmatic hernia: a report from the Congenital Diaphragmatic Hernia Study Group. J Pediatr Surg. 1998; 33:1004–1009.
19. Pierro A. Hypercapnia and acidosis during the thoracoscopic repair of oesophageal atresia and congenital diaphragmatic hernia. J Pediatr Surg. 2015; 50:247–249.
20. Yang EY, Allmendinger N, Johnson SM, Chen C, Wilson JM, Fishman SJ. Neonatal thoracoscopic repair of congenital diaphragmatic hernia: selection criteria for successful outcome. J Pediatr Surg. 2005; 40:1369–1375.
21. Putnam LR, Gupta V, Tsao K, Davis CF, Lally PA, Lally KP, et al. Factors associated with early recurrence after congenital diaphragmatic hernia repair. J Pediatr Surg. 2017; 52:928–932.
22. Kocaturk CI, Sezen CB, Aker C, Kalafat CE, Bilen S, Kutluk AC, et al. Surgical approach to posterior mediastinal lesions and long-term outcomes. Asian Cardiovasc Thorac Ann. 2017; 25:287–291.
23. Park T, Jung K, Kim HY, Jung SE, Park KW. Thoracoscopic management of a communicating bronchopulmonary foregut malformation in a 23-month-old child. J Pediatr Surg. 2012; 47:e21–e23.
 XML Download
XML Download