

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
Recent data suggest that monotherapy with a broad-spectrum antibiotic may be as efficacious as, and potentially less costly than, standard multi-drug therapy. We compared mono-therapy with intravenous piperacillin-tazobactam (PT) with multi-drug therapy with cefotaxime and metronidazole (CM) in aspect of postoperative complications and hospital stay.
Methods
We reviewed the hospital records and medical costs of the pediatric patients who were managed for perforated appendicitis between April 2013 and May 2014 retrospectively.
Results
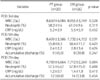
Forty-six patients with laparoscopic appendectomy for perforated appendicitis were included in our study. PT group was 20 and CM group was 26 patients. On admission, there were no significance in sex distribution, duration of symptoms, leukocyte count, and CRP levels. At postoperative third, fifth, and seventh day of each regimen, PT group have no statistical difference with CM group in leukocyte count, percentage of neutrophil, and CRP. There was no difference in abscess formation rate, wound infections, and hospital stay between two groups. There was only one patient who was readmitted with elevation of CRP and leukocyte count in CM group.
Figures and Tables



References
1. Williams RF, Interiano RB, Paton E, Eubanks JW, Huang EY, Langham MR, et al. Impact of a randomized clinical trial on children with perforated appendicitis. Surgery. 2014; 156:462–466.
2. Zerem E, Imamović G, Ljuca F, Alidžanović J. What is the optimal treatment for appendiceal mass formed after acute perforated appendicitis. World J Gastroenterol. 2012; 18:1849–1850.
3. Bauer T, Vennits B, Holm B, Hahn-Pedersen J, Lysen D, Galatius H, et al. Antibiotic prophylaxis in acute nonperforated appendicitis. Ann Surg. 1989; 209:307–311.
4. Pieper R, Kager L, Näsman P. Acute appendicitis: a clinical study of 1018 cases of emergency appendectomy. Acta Chir Scand. 1982; 148:51–62.
5. Browder W, Smith JW, Vivoda LM, Nichols RL. Nonperforative appendicitis: a continuing surgical dilemma. J Infect Dis. 1989; 159:1088–1094.
6. Bates T, Touquet VL, Tutton MK, Mahmoud SE, Reuther JW. Prophylactic metronidazole in appendicectomy: a controlled trial. Br J Surg. 1980; 67:547–550.
7. Hopkins JA, Lee JC, Wilson SE. Susceptibility of intra-abdominal isolates at operation: a predictor of postoperative infection. Am Surg. 1993; 59:791–796.
8. Curran TJ, Muenchow SK. The treatment of complicated appendicitis in children using peritoneal drainage: results from a public hospital. J Pediatr Surg. 1993; 28:204–208.
9. Gollin G, Abarbanell A, Moores D. Oral antibiotics in the management of perforated appendicitis in children. Am Surg. 2002; 68:1072–1074.
10. Lund DP, Murphy EU. Management of perforated appendicitis in children: a decade of aggressive treatment. J Pediatr Surg. 1994; 29:1130–1134.
11. Fishman SJ, Pelosi L, Klavon SL, O'Rourke EJ. Perforated appendicitis: prospective outcome analysis for 150 children. J Pediatr Surg. 2000; 35:923–926.
12. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004; 240:205–213.
13. Newman K, Ponsky T, Kittle K, Dyk L, Throop C, Gieseker K, et al. Appendicitis 2000: variability in practice, outcomes, and resource utilization at thirty pediatric hospitals. J Pediatr Surg. 2003; 38:372–379.
14. Chen C, Botelho C, Cooper A, Hibberd P, Parsons SK. Current practice patterns in the treatment of perforated appendicitis in children. J Am Coll Surg. 2003; 196:212–221.
15. Rice HE, Brown RL, Gollin G, Caty MG, Gilbert J, Skinner MA, et al. Results of a pilot trial comparing prolonged intravenous antibiotics with sequential intravenous/oral antibiotics for children with perforated appendicitis. Arch Surg. 2001; 136:1391–1395.
16. Nadler EP, Reblock KK, Ford HR, Gaines BA. Monotherapy versus multi-drug therapy for the treatment of perforated appendicitis in children. Surg Infect (Larchmt). 2003; 4:327–333.
 XML Download
XML Download