

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The patella is known to have the thickest articular cartilage and it is most commonly the site of degeneration. It is subcutaneously placed, which makes it prone to the trauma and it can be affected by any systemic skeletal disorder. Since it takes part in the formation of knee joint, the patellar disorders are often confused for various intra capsular derangements of knee joint. It is very obvious that the study of patella has various clinical implications. The success of total knee arthroplasty (TKA) or patello femoral arthroplasty (PFA) depends on obtaining the suitable patellar implant size. The conventional methods of planning the implant include the intraoperative measurement of the patella, which may sometimes go for an error due to the diseased joint. The gender variability in the dimensions of patella may also have implications for implant design and functional outcome after the successful PFA or TKA. It is well known that, there is significant difference in the morphometry of the knee joint between the Asian and Caucasian population [1]. Unfortunately, most of the commercially available knee prosthesis for TKA or PFA are designed based on the dimensions from the Caucasians, which may not be suitable for the Asians [2345]. In this context, the present study aims to address the clinical need for the implants based on the population and between male and female patella. The goal of the present investigation was to provide the morphometric data of the patella bone and to describe the gender variations of the patella bone in South Indian population by studying the magnetic resonance imaging (MRI) films.
Materials and Methods
The present investigation is a retrospective study, performed between 2013 and 2015, where a total of 140 patients were studied. The randomly selected knee joint MRI films among 70 males and 70 females, aged between 20 and 70 years were included. The patients belonged to the teaching hospital of our institution which is located in South India. The patients with congenital anomaly, severe trauma, surgery, acute patellar dislocation, patellar fracture, knee joint tumour, and rheumatoid arthritis were excluded from the present study. The present study has the approval from the ethics committee of our institution.
The computed tomography (CT) scan is good for the bone window, like studying the patella. But unfortunately, we did not get enough CT scan films to perform this investigation. This is because CT scan is rarely done in comparison to the X-ray and MRI of the knee and MRI delineates the cartilage boundary better. However, the cartilage is not included in the measurements of the present study because of the age based variation. The wear and tear also cause variation in the measurements of the cartilage.
The MRI films have been performed with a Signa 1.5 T MRI System (GE Healthcare, Milwaukee, WI, USA). Every patient was advised to lie down in supine position with the knee extended during the procedure. The T2 weighted axial magnetic resonance (MR) images of knee joint with slice thickness of 4 mm were studied. The mid transversal layer of the axial MRIs [6], which allowed the visualisation of maximum transverse diameter were examined to assess the patellar anatomic morphology. The following parameters were measured in the present study.
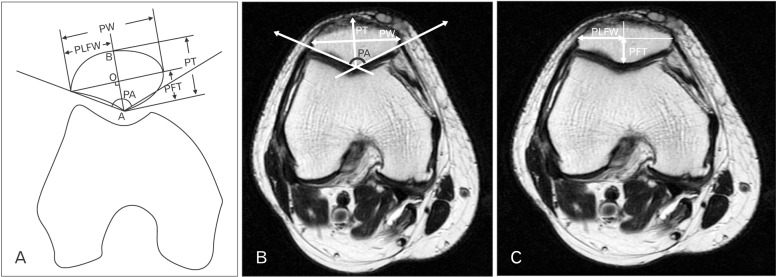
1. Patellar angle (PA): the angle of lateral and medial patellar facets, with the point of the central ridge of patella as the zenith (Fig. 1A, B).
2. Patellar width (PW): the distance between the most medial and lateral ends of the patella (Fig. 1A, B).
3. Patellar thickness (PT): the distance between the patellar central ridge point (A) to the anterior point (B) of patella (a perpendicular line was put from the patellar central ridge point [A] to the line PW, “line a”). The patellar anterior point (B) is defined as the intersection point of line a, and the patellar anterior bony surface. The central point of patella (O) is defined as the point of intersection between line a, and line PW (Fig. 1A, B).
4. Patellar lateral facet width (PLFW): the distance of most lateral point of patella from the central point of patella (Fig. 1A, C).
5. Patellar facet thickness (PFT): the distance of patellar central ridge point to the central point of patella (Fig. 1A, C).
6. Patellar lateral facet ratio (PLFR=PLFW/PW): the PLFW was divided by the PW.
7. Patellar relative thickness (PRT=PT/PW): the PT was divided by the PW.
8. Patellar facet thickness ratio (PFTR=PFT/PT): the PFT was divided by the PT.
Results
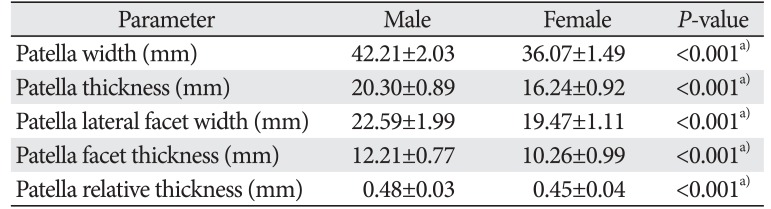
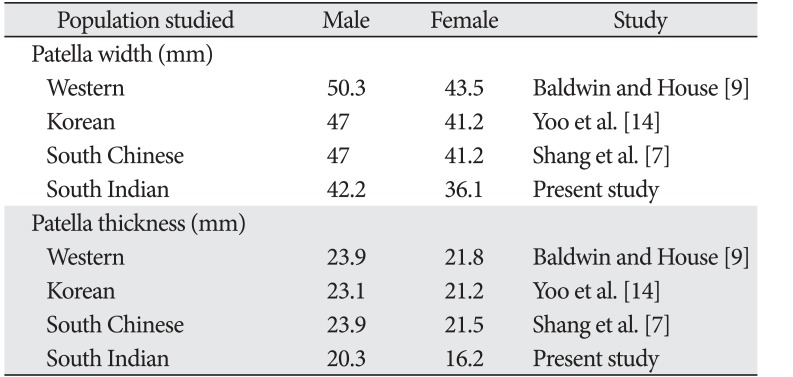
Among the dimensions, the angle, the width, the thickness, the lateral facet width, the facet thickness, the relative thickness and the facet thickness ratio of the patella were exhibited statistically highly significant (P≤0.001) sexual dimorphism (Tables 1, 2, 3). The only patellar parameter which was not significant statistically was the PLFR (Table 3). The mean value was higher in males than in females except for the lateral facet ratio (PLFW/PW) and the facet thickness ratio (PFT/PT) of patella as shown in Tables 1, 2, 3. The comparison of standard deviation suggests that the males exhibit more variability than females in all the measurements of patella except the thickness, facet thickness, relative thickness (PT/PW) and facet thickness ratio (PFT/PT) as shown in Tables 1, 2, 3. The width and thickness of the patella from the present study was compared with the data from literature from Western, Korean, and South Chinese population. This comparison is being represented in Table 4.
Discussion
The morphometry of patella can be performed by direct or indirect measurements [7]. One among the direct measurements, is with the dried bones or skeletal remains [58]. The other one being the intraoperative measurement performed by the operating surgeon by using a caliper [91011]. However, it is hard to procure the sufficient quantity of the dry bones or the patients who are undergoing the PFA or TKA surgeries, to perform the detailed research analysis. Fortunately, it is possible that the indirect in vivo measurements can be performed. One among the indirect in vivo measurements is by measuring the radiographic images using a digital ruler. The radiographic studies also provide an added advantage of having digital data available for the future reference and research. In this present study, we adopted the indirect method by using the MRI films, and all the measurements in this present study were collected noninvasively. However, the present study has few limitations like the 3D models of patella, which were not reconstructed. The 3D MRI models would have given the better results in the measurements. Recently, a new measurement was recommended based on the 3D models reconstructed by the computer software, but the 3D model did not include the cartilage which became a major limitation [71213]. So, the use of MRI films proves to be a quick, accurate, inexpensive, and noninvasive method to get the morphometric in vivo measurements of the patellofemoral joint.
During the analysis of the patellar parameters from MR images in the present study, the angle, width, thickness, width of lateral facet, thickness of facet, relative thickness and the ratio of facet thickness exhibited the high statistically significant sexual dimorphism (P≤0.001). The only patellar parameter which was not significant statistically, was the PLFR. It was observed that the male patellae had larger geometrical dimension than the female patellae. Similar findings were observed by Shang et al. [7] from the Chinese population, Yoo et al. [14] from Korean population and Baldwin and House [9] from the Western population. In the present study, the mean value was higher in males than females for all the patellar parameters, except the lateral facet ratio (PLFW/PW) and facet thickness ratio (PFT/PT). The males exhibited more variability than females in all measurements of patella except the PT, PFT, PRT (PT/PW) and PFTR (PFT/PT).
The mean PA in the present study was found to be 127.23°±4.76° in males and 125.01°±2.87° in females. Another study from the Western population by McHale et al. [15] showed similar trend of PA among the male and female genders. It was reported that the patella of Asian population are thinner and smaller than that of the Western subjects [711]. This fact is confirmed in the present study for a South Indian population. The present study showed the mean PW to be 42.21 mm in males and 36.07 mm in females, which were smaller than reported by Baldwin and House [9] for the Westerns, 50.3 mm in males and 43.5 mm in females. Our South Indian morphometric data of the patella was also smaller, than the reports from Southern Chinese and Korean population, 47.01 mm in males and 41.25 mm in female [71114]. The analysis of the mean PT was found to be smaller than that of the Western, Korean, and South Chinese population [7913]. In the present study, the PT was 20.30±0.89 mm for males and 16.24±0.92 mm for females. Baldwin and House [9] reported a PT of 23.9 mm in males and 21.8 mm in females. Yoo et al. [14] observed the value as 23.1 mm in males and 21.2 mm in females, which was close to the values reported by Shang et al. [7], 23.91 mm for males and 21.52 mm for females. Thus it is obvious that the South Indian female is found to have the thinnest patella of mean value 16.24 mm, in comparison to the Western, Korean, and South Chinese population. This becomes an important variable to be considered, while assessing the South Indian female for patellofemoral disorders and designing the patellar prosthesis implant. The optimum thickness of patella is essential to the success of the knee arthroplastic surgery.
The TKA is the best surgical procedure; however, the operating surgeons are challenged by the patellofemoral joint derangement, following it [16]. The postoperative complications remain as the disability and the thickness of patella being the most important factor [16]. A thinner patella can decrease the friction, but can also lead to the stress fracture and the instability. The increased PT may increase the quadriceps movement at a low flexion angle of the knee; however, it reduces the range of knee movements, which can cause patellar subluxation. The thicker or thinner patella has a lesser contact area than the normal size patella. Due to all these concepts, it would be a great decision to identify the race, geography, gender, and age specific thickness of patella during the procedure of prosthesis implantation. It is believed that the morphometric data of the present study can help in the preparation of the prosthesis implants size for the South Indians.
The width/thickness ratio of the patella was assessed by Iranpour et al. [13] to establish the optimum size of the prosthesis implant size during the knee arthroplasty. The present study also measured the PRT, the ratio of thickness to the width. This can also be used as a guide to estimate the thickness of the premorbid patella. The present study observed that the PRT was found to be 0.4817 and 0.4513, respectively, in males and females with a statistically high significance (P<0.001). According to Bogen [17], the patients with dislocation have conspicuously smaller patella. This fact predisposes the South Indian females to a greater risk for the patellar dislocation. South Indian females can be advised to avoid certain sudden movements to prevent them from dislocating the patella.
The dimensions of the articulating facet of patella included its thickness, width of lateral facet, ratio of lateral facet and the thickness ratio of lateral facet. The present study observed that the PFT was 12.21 mm in males and 10.26 mm in females with a statistically high significance (P<0.001). The PLFW revealed a mean value of 22.59 mm in males and 19.47 mm in females. This was smaller compared to the South Chinese population, 26.91 mm in males and 23.30 mm in females, while the same dimensions were measured in the Western was 29.7 mm in males and 25.3 mm in females [79]. Yang et al. [6] reported that the lesions of patellar femoral cartilage are higher if the patella has the dominant lateral articular facet. This can be calculated with the PLFR, which was found to be 0.5358 in males and 0.5406 in females in the present study. The PFTR (the ratio of facet thickness to thickness of patella) was 0.6024 in males and 0.6319 in females in the present study, with highly significant difference (P=0.001). We believe that all the significant values determining the patellar facet should be considered, while designing the gender wise patellar prosthesis implant to ensure the successful functional outcome during the TKA or PFA in South Indian population.
The patella being the largest sesamoid bone in humans, act as the key factor in the extensor mechanism of the lower extremity. The patella has also got its medicolegal implications as it was used in many studies as a sex assessor with the highest accuracy of 95%. This is the bone used for the sex determination [818192021]. So, the morphometric data of the present study are also important to the forensic science anthropologists and researchers.
The present study performed the in vivo morphometry of the patella bone from the South Indian population by using the axial MR images. The statistical analysis revealed that the males have a larger patella than the females. Seven among the eight morphometric parameters of the patella depicted the significant gender variation. The dimensions of the South Indian patella are smaller and thinner than those of Western. Compared with the previous studies among the Western, Chinese, and Korean population, the patella in our study was smaller and thinner.
The present investigation has determined the important dimensions of the patella bone in the South Indian population. The morphometric data of the present study could be useful to the clinician while dealing with the cases of the anterior knee pain and disorders of the patellofemoral joint. This preliminary study, which is the representative of the South Indian population, can provide the guidelines to manufacture the prosthetic implants of the patella. This is clinically essential since the South Indian population have smaller anthropometric measurements of patella than the Western population. The data are enlightening especially to design the gender and racial specific prosthetic implant. We believe that this method of in vivo MRI morphometry makes it easy to obtain the anatomical data with high accuracy and reproducibility.


 XML Download
XML Download