

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Intrathoracic rib is a very rare congenital disorder. It is usually silent, and discovered accidentally; its understanding can prevent mistake with other of thoracic diseases like as a lung consolidation, pleural lesion, peripheral lung parenchymal lesions, and bony lesion during imaging diagnostic techniques. It may arise from a rib or a vertebra, and sometimes it may be associated with vertebral anomalies and are usually unilateral [1 2].
Here, we present a unique case of intrathoracic rib in a 3-year-old boy with an unusual appearance of an intrathoracic rib, which is originating from an inferior-lateral portion of a second rib, without articulation with the vertebrae through the use of helical computed tomography (CT) scan with 3D reconstructions.
Case Report
We describe the discovery during a chest CT scan was done in a 3-year-old boy for examination of symptoms of upper respiratory tract infection as he complained of cough, high grade fever, and chest pain for one month. The patient had no other medical history and chest trauma.
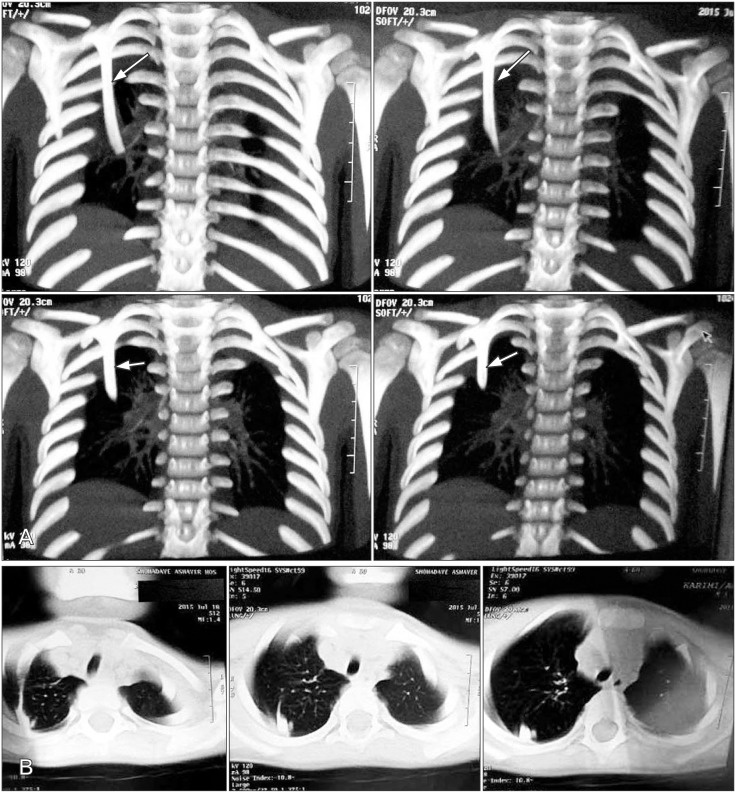
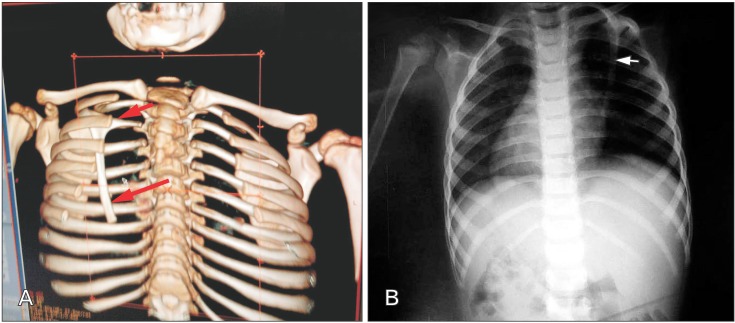
For further examination, CT scan of the chest was done and 3D and multiplanar reconstructions were performed. Helical CT with 3D reconstructions (GE Light Speed 16-Slice Spiral CT Scanner, General Electric, Milwaukee, WI, USA; 120 kV, average mAs 98 [dose modulation], pitch 0.828, collimation 0.5-mm reconstructed 2.5-mm intervals) in the coronal and axial plane, displayed a right intrathoracic rib with unusual characteristics (Fig. 1A, B).
The ossific, soft-tissue thin, short, and obliquely oriented structure with no identifiable medullary cavity originating from the middle part of inferior border of the right second rib appears to be an accessory second rib coursing into the chest cavity and migrates inferior-interior toward seventh rib. No vertebral alteration was observed (Fig. 2A, B). The subject's clinical history reflects prior respiratory complaints, indicating that the congenital anomaly may have effect on respiratory physiology and lung morphology that need more evaluation.
Discussion
Intrathoracic ribs are uncommon congenital variation where an incomplete supra- or normonumerary rib follows an abnormal course in the intrathoracic cavity and may originate from a vertebra or a rib [3]. To our knowledge, 50 cases of intrathoracic rib have been appeared in the literature so far after first reported in 1947 [345678910]. The condition was first described by Lutz et al. [11] in a 25-year-old woman based on radiological observations, and since then there have been 50 reported cases in the literature. Approximately one-third of reported cases are in children; we found some of those to be demonstrated by cross-sectional imaging [9 12].
Intrathorasic ribs are usually without symptoms and are found accidently during examination in autopsies and diagnostic imaging tests (radiographic, CT scan) and are affected in up to 1% of the general population. This abnormality can be seen throughout a range of ages from 3 to 79 years, is independent of sex, more common unilateral, generally on the right side and incline to affect only one rib. Intrathoracic ribs usually origin from the posterior and inferior aspect of the normal rib or vertebral body [12].
The origin of the variation ribs is unknown. During embryogenesis incomplete fusion between adjacent sclerotomes and also alteration of intrathoracic or extrathoracic pressure in the embryo [13141516], resulting in formation of intrathoracic ribs between fourth week and sixth week of fetal life. Although in some case they have been associated with genetic alteration.
Recently, classification of abnormal ribs has been proposed by Kamano et al. [3] according to the location and the origin of ribs and explains four types type IA and IB, those articulated with the vertebral body, latter originate from the posterior part of the rib. Type II is bifid intrathoracic ribs and type III is intrathoracic ribs caused by a costal depression into the thoracic cavity. Our case is IB since the unusual rib is originated from second rib.
In summary, intrethoracic ribs should be considering it in the differential diagnosis of pleural and lung disorders and other peripheral lung parenchymal lesions. CT scan is great method to show its presence. Some authors have reported inthrathoracic ribs via CT scans and three-dimensional reconstructions [16]. So, discovering of this anomaly may prevent of extra evaluation and investigation.
In some cases it can be associated with other variation like as bone dysplasi, cervical rib, dysplasia and malformations of the thoracic vertebrae as far as the diaphragm.
Radiology and CT are the most important tool for diagnosis of this abnormality. In our case, the helical CT scan revealed a thin styloid-like osseous structure origining from the anterior aspects of the middle part of second rib.
 XML Download
XML Download