

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Prostate cancer is the most common cancer in middle-aged and elderly men after lung cancer with the prevalence of 25.3 per 10,000. The previous studies have shown that one man in six will suffer from this cancer during his lifetime. Genetic, hormonal, and environmental factors are known to be involved in the incidence of this cancer. It is most prevalent in the Northern Europe and Africa, and the least incidence is reported in the Asian population [12].
Screening, diagnosis, and treatment in the early stages of prostate cancer can improve the patients' life expectancy and quality of life and decrease morbidity and mortality [3]. Digital rectal examination and serum prostate specific antigen (PSA) measurement are the main diagnostic methods [4].
PSA is a proteolytic enzyme released by normal and neoplastic prostate cells. Any damage to prostate, including hyperplasia, adenocarcinoma, cystoscopy, prostatitis, and senility, has been reported to increase the serum level of this antigen; however, this antigen is widely used to diagnose prostate cancer [567].
This specific antigen is in a higher level in patients with prostate cancer although it does not necessarily indicate affliction to it as high level of PSA is also observed in many men with benign hyperplasia of prostate and urinary tract infections. To confidently diagnose prostate cancer, PSA measurement is followed by further tests including magnetic resonance imaging, computed tomography, ultrasound, and prostate biopsy. However, about 25% of prostate cancer is not diagnosed after first biopsy [8].
The previous studies have shown that despite the negative result of biopsy, PSA level increases, but in a few percentages of gland lesions, the level of PSA does not increase.
Therefore, considering the restriction and the low diagnostic accuracy of screening methods, finding a reliable method of diagnosis is significant [9]. Recently, human leukocyte antigen-G (HLA-G) has been introduced as a tumor marker for breast cancer, lung cancer, skin cancer, ovarian cancer, and gastrointestinal cancer [10]. It is shown that the evaluation of HLA-G level in serum or plasma can increase specificity of diagnosis [111213].
The present study is an attempt to evaluate the level of this tumor marker in comparison with the pathological findings in patients suffering from prostate cancer and to assess its efficiency as a new biomarker for screening purposes.
Materials and Methods
The present descriptive-experimental study was carried out in Nowshahr Medical Diagnostic Institute (Feb 2014–Jan 2015). First, among the patients who had referred to the laboratory, those with prostate cancer who met the inclusion criteria were selected and informed about the study. Prior to biopsy procedure, all the participants wrote and signed the consent form and their familial history was elicited.
Inclusion criteria were patients with benign or acute prostate cancer, approval of the cancer stage by an oncologist and a pathologist, and no history of other diseases. Patients whose cancer stage was unknown were excluded from the study.
Participants were divided into three groups: group 1 included 26 patients with acute prostate cancer; group 2 included 26 patients with benign prostate cancer; and group 3, comprised of 26 healthy participants. Two milliliters of blood was sampled from each participant. After separating serum in sterilized condition, the levels of biomarkers were measured in the three groups using Human AHLA-G ELISA Kit (Elabscience-Biotechnology, Wuhan, China). The data was analyzed by one-way analysis of variance (ANOVA) with significance set at P<0.05.
Results
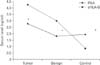
The statistical analyses revealed that the levels of PSA in malignant group, benign group, and control group were 3.45, 2.88, and 2.31, respectively, showing no statistically significant different between the groups (P<0.05) (Fig. 1). The highest level of PSA was found in the malignant group. The results of measuring HLA-G level were 1.68, 1.59, and 0.83 in malignant tumor group, benign tumor group, and control group, respectively, demonstrating a statically significant different between the three groups (P<0.05) (Fig. 2). The highest level of HLA-G was found in the group with malignancy. Also, when the mean of the serum level of PSA was compared with that of the serum level of HLA-G, no significant difference was observed between the three groups (P<0.05) (Fig. 3).
Discussion
The aim of the present study was to evaluate serum level of HLA-G as an efficient tumor marker in screening and diagnosis of patients with prostate cancer and also to compare HLA-G and PSA in terms of their biomarker role. The serum level of PSA was abnormal in patients who suffered from prostate cancer, but no significant difference was observed between the malignant group and benign group with regard to the level of this biomarker. Moreover, the mean of the serum level of HLA-G was found to be high in the three groups. The results of the statistical analyses showed that there is a significant difference between the three groups of study concerning the serum level of HLA-G with the highest level belonging to the malignant tumor group and the least level to the control group; therefore, it can be stated that there is a positive correlation between the serum level of HLA-G and the stage of cancer. Evaluation of PSA level is routinely used in laboratories for screening prostate cancer where increase in the serum level of this antigen is interpreted as increase in the severity of the disease, yet according to our findings, there is no correlation between the disease, cancer stage, and the serum level of PSA.
HLA-G is one of the molecules of MHC I that plays the roles of immunosuppression and regulatory of natural killer cell and dendritic cell T-cell [10]. Previous studies have reported on the clinical linkage between an increase in expression of HLA-G in diseases such as cancer, viral infection, pregnancy, organ transplants, autoimmune disease, and inflammations. HLA-G expression were found, for the first time, in trophoblastic cell in chorion playing fundamental roles in protecting fetus against mother's immune system, survival of the fetus, and early stages of placenta angiogenesis [13]. Also, HLA-G has been detected in people receiving allograft and tumor progression in several cancers [14]. Similar to our findings, Wang et al. [15] has reported that there is positive a correlation between expression of HLA-G and size of glioma tumor. In another study, Guo et al. [16], after evaluation of the expression of HLA-E or HLA-G in patients with colorectal cancer, concluded that there is a direct relationship between HLA-G or HLA-E and metastasis rate and mortality.
In 2006, expression of HLA-G1, -G2, -G5, and -G6 were evaluated in normal prostate tissue, prostate hyperplasia, and prostate adenocarcinoma by Langat et al. [17]. They reported that HLA-G5 exists in prostate tissue and it increases in tissue secretion of prostate adenocarcinoma.
According to findings of the present study, the evaluation of serum level of HLA-G can be used as a novel and an easy method for screening, diagnosis, and staging of prostate cancer, as early diagnosis of prostate cancer can decrease morbidity and mortality and increase life expectancy in the patients.


 XML Download
XML Download