

Introduction
Pulmonary artery hypertension (PAH) is a progressive chronic disease with a high mortality rate [1]. PAH has a complex disease mechanism. Its cardinal signs include an elevation of pulmonary artery pressure, right ventricular (RV) hypertrophy, and arteriolar wall remodeling [2]. Increased pulmonary vascular resistance and over-proliferation of pulmonary artery endothelial cells lead to remodeling of pulmonary vasculature [345]. They also cause damage to the pulmonary microvasculature and impact blood flow from heart to lungs [67]. Although current treatments may prolong and improve quality of life of patients, the long-term prognosis for PAH remains poor with survival of 2 to 3 years since the time of diagnosis [1].
Prostaglandin E1 (PGE1, Alprostadil) is a compound with vasodilatory, anti-inflammatory, anti-aggregatory, and anti-proliferative properties [8910]. PGE1 has been approved by the U.S. Food and Drug Administration (FDA) for the treatment of erectile dysfunction in men and patent ductus arteriosus in newborns. PEG1 has been investigated as treatment for various cardiopulmonary disorders, especially for pulmonary arterial hypertension [11121314]. However, the clinical utility of PGE1 has been limited due to its chemical instability and extremely hydrophobic nature which results in low drug absorption and poor bioavailability. Recently, there has been renewed interest in the use of PGE1 in cardiac and lung transplantation. Using target organ infusion protocols can circumvent the extensive first pass metabolism of PGE1 by the lungs and prevent the decreased bioavailability and clinical efficacy of PGE1 infused systemically [1516171819].
It has been demonstrated that PGE1 can improve pulmonary hemodynamics and clinical outcomes of patients with PAH [20]. However, the long-term effect of PGE1 on rats with monocrotaline (MCT)-induced PAH has not been investigated. Therefore, the aim of this study was to evaluate the effect of continuous intravenous PGE1 on hemodynamics and long-term outcomes of rats with MCT-induced PAH. To determine changes in pulmonary haemodynamics, RV hypertrophy, pathology, and protein expressions, we used immunohistochemical staining and western blot analysis to understand whether PGE1 treatment could reduce the development of PAH in the model.
Go to : 
Materials and Methods
Animals
Six-week-old male Sprague-Dawley rats were used. All rats were housed in climate-controlled conditions with a 12-hour light/12-hour dark cycle, and had free access to food and water. All animal experiments were approved by the appropriate Institutional Review Boards of the Seoul National University Bundang Hospital (BA1703-219/018-01) and conducted in accordance with National Institutes of Health Guide for the Care Use of Laboratory Animals (NIH publication No. 86-23, revised in 1996).
PAH rat model
PAH was induced by subcutaneous injection of 60 mg/kg MCT (Sigma-Aldrich, St. Louis, MO, USA) dissolved in 0.5 N HCl. Rats were assigned into the following groups: (1) control group (C group; 20 rats), vehicle injection with normal diet; (2) monocrotaline group (M group; 20 rats), MCT injection with normal diet; and (3) PGE1 group (20 rats), MCT injection+PGE1 injection with normal diet. These animals were sacrificed at 7, 14, 21, and 28 days (each group, n=5) after MCT administration (Fig. 1). Tissues were removed and immediately frozen at −70℃ for enzyme analysis.
Drug delivery
Osmotic infusion pump (Alzet Model 2ML-1, ALZA Corp., Palo Alto, CA, USA) was utilized as drug delivery system as described previously [21]. Alzet 2ML-1 is a fully implantable and osmotically driven pump. It can deliver 2 ml over a period of 7 days at a constant rate of infusion. PGE1 (Lot U-10136, Upjohn, Kalamazoo, MI, USA) was dissolved in absolute ethanol dried over sodium sulfate and added to the pump to yield an infusion rate of 0.1 pg/kg/min. This dose was chosen based on previous experiment showing that animals receiving it could tolerate high doses of PGE1 [22]. Based on pilot studies, PGE1 was found to be stable in the pump for 7 days at pH 7.4.
Determination of the organ weights and right hypertrophy index
The rats were weighed and observed for general appearance during the study period. The animals were sacrificed at the scheduled time. The wet weights of excised RV, left ventricle (LV) plus interventricular septum (IVS) (LV+IVS) were measured. The RV to LV+IVS ratio [RV/(LV+IVS)] was used to determine the right hypertrophy index (RVI). The standard of RV hypertrophy was defined as an RVI>0.33 [23].
Pulmonary haemodynamics
Rats were anaesthetized by intraperitoneal injection of urethane and secured on a surgical stage. An 8-mm-long right internal jugular vein was isolated and ligated at the distal end. The vessel was cut at the proximal end of ligation. A catheter filled with heparin saline was rapidly inserted along the incision and slowly advanced for about 5 cm to enter the pulmonary artery. The standard of pulmonary hypertension was defined as systolic pulmonary artery pressure (SPAP) >50 mm Hg [23]. Hemodynamic parameters were recorded at baseline and at 7, 14, 21, and 28 days.
Histologic findings of pulmonary arteries
Heart and lung tissues were fixed with 10% buffered formalin and then embedded in paraffin. Sections were performed by 4-µm-thick hematoxylin-eosin stains to evaluate histopathologic changes of pulmonary blood vessels. The small pulmonary artery wall thickness was expressed as follows: % wall thickness.
Masson trichrome staining
Masson trichrome staining was carried out in accordance with well-characterized protocols. Briefly, heart and lung tissue sections were deparaffinized and hydrated in distilled water prior to a 1-hour treatment in Bouin's fixative (Catalog #NC9674780, Richard-Allan Scientific, Carlsbad, CA, USA) at 56℃. Sections were washed in running distilled water until clear, and then stained in Weigert's iron hematoxylin (Catalog #NC9231529, Richard-Allan Scientific) for 10 minutes. Following a 10-minute wash in running water, sections were stained in Biebrich scarlet-acid fuchsin (Catalog #NC9424144, Richard-Allan Scientific) for 2 minutes. Sections were rinsed in distilled water followed by a 10-minute differentiation in phosphomolybdic-phosphotungstic acid (Catalog #NC9443038, Richard-Allan Scientific). Aniline blue (Catalog #NC9684104, Richard-Allan Scientific) was used as a counterstain for 10 minutes, and then sections were differentiated in 1% acetic acid for 3 minutes. Sections were dehydrated through a series of graded alcohols back to xylene, and then coverslipped and sealed using Cytoseal XYL (Richard-Allan Scientific).
Immunohistochemistry
Excised lung tissues were incubated overnight in 10% buffered formalin. Four-micrometer-thick sections were cut from paraffin embedded tissue blocks, deparaffinized in xylene, and rehydrated in graded alcohol solutions (70%–100%). Heat antigen retrieval was achieved by boiling the tissue sections in antigen retrieval solution in pH 6.0 or pH 9.0 (Dako, Carpinteria, CA, USA) for 10 minutes in a microwave prior to incubation at 4℃ overnight with primary antibodies against endothelin-1 (ET-1; Abcam, Cambridge, MA, USA). After incubation with the appropriate biotinylated secondary antibodies for 30 minutes at 4℃ and subsequently with streptavidin (Dako, Kyoto, Japan), color development was done using diaminobenzidine (DAB) as a chromogen and counterstained with hematoxylin.
In situ terminal deoxynucleotidyl transferase-mediated deoxyuridine triphosphate nick-end labeling technique assay for lung cell apoptosis
Apoptotic cells in the lung tissue sections were detected by the terminal deoxynucleotidyl transferase-mediated deoxyuridine triphosphate nick-end labeling technique (TUNEL) using a commercial apoptosis kit (TACS TdT Kit, R&D Systems Inc., Minneapolis, MN, USA), according to the supplier's instructions. In brief, the lung tissue sections were de-paraffinized with xylene and ethanol and rinsed with phosphate buffered saline (PBS). The sections were then treated with proteinase K in PBS followed by quenching of endogenous peroxidase. A biotinylated dNTP mix was added to the 3′-OH ends of DNA by terminal deoxynucleotidyl transferase (TdT). After incubating with streptavidin-horseradish peroxidase, the sections were stained with DAB and counterstained with methyl green. Finally, the sections were dehydrated in ethanol, cleared with xylene, and mounted with coverslips in a permanent medium. According to the supplier's instructions, experimental controls included for the assay were TACS-nuclease–treated thyroid tissue sections as the positive control and the omission of the TdT reaction step as the negative control.
Western blot analysis
The tissue was homogenized in 10 mM Tris HCl buffer, pH 7.4 containing 0.5 mM EDTA, pH 8.0, 0.25 M sucrose, 1 mM phenylmethylsulfonyl fluoride, 1 mM Na4VO3 and a protease inhibitor cocktail (Roche-Boehringer-Mannheim, Mannheim, Germany). After centrifugation, the supernatant was subjected to sodium dodecyl sulfate polyacrylamide gel electrophoresis (SDS-PAGE). Samples equivalent to 25 µg of protein content were loaded and size-separated in 8%–12% SDS-PAGE. The proteins on the acrylamide gel were transferred to a polyvinylidene difluoride membrane (Millipore, Bedford, MA, USA) at 400 mA in a transfer buffer containing 25 mM Tris and 192 mM glycine, pH 8.4. The nitrocellulose membranes was blocked in Tris-buffered saline with 5% non-fat dry milk at room temperature for 1 hour in 0.1% Tween 20 and incubated with the appropriated primary antibodies, including anti-ET-1 and anti–endothelin receptor antagonist (ERA) (Santa Cruz Biotechnology Inc., Santa Cruz, CA, USA) and anti-actin (Santa Cruz Biotechnology Inc.), at 4℃ overnight. The membranes were then incubated with horseradish peroxidase–conjugated secondary antibody (Cell Signaling Technology Inc., Danvers, MA, USA) for 1 hour at room temperature. After washing, the membranes were visualized by a chemiluminescent ECL-detection kit from GE-Healthcare (Piscataway, NJ, USA).
Statistical analyses
Results were expressed as the mean±standard deviation. Differences between all other parameters for the three groups were evaluated by ANOVA followed by multiple-group comparisons. An unpaired two-tailed t test and Mann-Whitney test were used, and a P-value of <0.05 was considered statistically significant. SPSS version 14.0 for windows (SPSS Inc., Chicago, IL, USA) was used for all statistical analyses.
Go to :
Results
Organ weight
RV weight of the M group was increased at 21 and 28 days after MCT administration. Weights of LV+IVS were not significantly different among C, M, and PGE1 groups. RV/LV+IVS ratios were significantly increased at 14, 21, and 28 days in the M group compared to those in the C group. However, RV/LV+IVS ratios were significantly decreased at 21 and 28 days in the M group compared to those in the PGE1 group. Weights of LV+IVS were significantly lower in the M group and the PGE1 group compared to those in the C group at 21 and 28 days. Heart weights were significantly increased in the M group compared to those in the C group at 21 and 28 days. However, heart weights were significantly decreased in the PGE1 group compared to those in the M group at 21 and 28 days (Table 1).
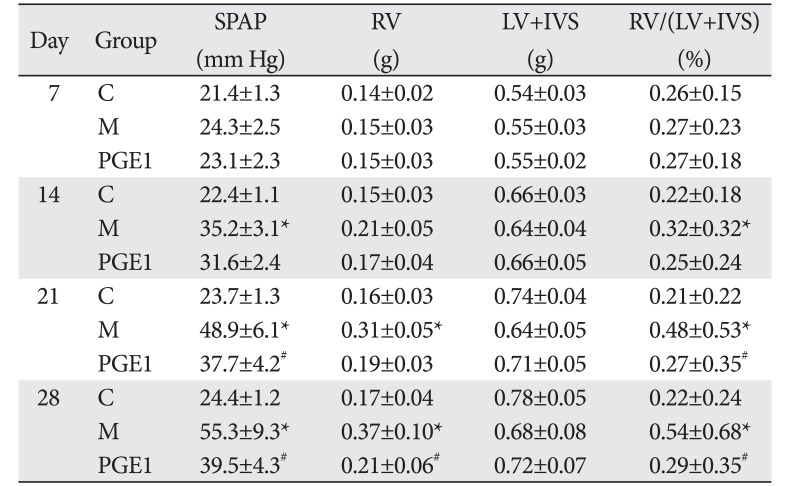
Table 1
Changes of SPAP and organ weights after PGE1 treatment in PAH rats
Values are presented as mean±SD. SPAP, systolic pulmonary artery pressure; PGE1, prostaglandin E1; PAH, pulmonary arterial hypertension; RV, right ventricle; LV, left ventricle; IVS, interventricular septum; C, control; M, monocrotaline. *P<0.05 compared with the C group, #P<0.05 compared with the M group.
![]()
Changes in SPAP after PGE1 treatment in PAH rats
Mean SPAP values were significantly increased in the M group compared to those in the C group at 14, 21, and 28 days. SPAP values were significantly decreased in the PGE1 group compared to those in the M group at 21 and 28 days (Table 1).
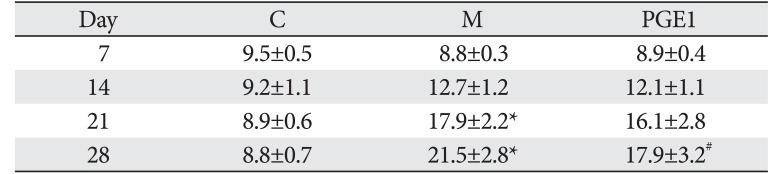
Medial wall thickness of the pulmonary artery
In the M group, the ratio of medial thickening to the external diameter of the pulmonary artery was significantly increased from 28 days compared to that in the control group. In the PGE1 group, the ratio of medial thickening of the pulmonary artery was not significantly decreased compared to that in the M group (Table 2).
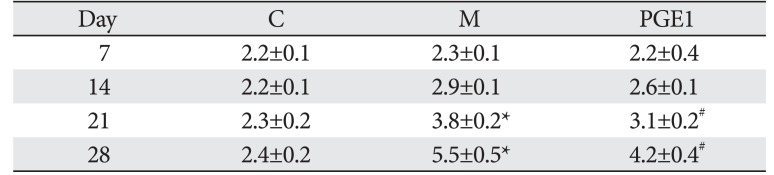
Number of muscular pulmonary arterioles
The number of muscular pulmonary arterioles was significantly increased in the M group compared to that in the C group. From 21 and 28 days, the number of muscular pulmonary arterioles was significantly decreased in the PGE1 group compared to that in the M group (Table 3).
Administration of PGE1 reduces RV and lung collagen deposition
To evaluate the effect of PGE1 treatment on the development of cardiac fibrosis, lung fibrosis, and remodeling, lung and RV samples were collected at 28 days after administration of MCT to determine histology patterns in the lung and RV. Results are shown in Figs. 2 and 3. After staining with Masson Trichrome, lung and RV sections showed more pronounced collagen deposition from animals with PAH compared to those in the control or PGE1 group (P=0.003 vs. C group, P=0.01 vs. M group; Fig. 2) (P=0.003 vs. C group, P=0.01 vs. M group; Fig. 3).
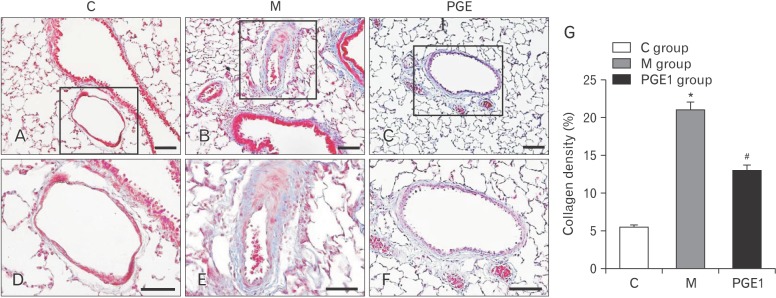 | Fig. 2Representative images of lung stained with Masson Trichrome from C group (A), M group (B), and PGE1 group (C) at 28 days following the injection of monocrotaline. Panels (D), (E), and (F) are high power views of panels (A), (B), and (C); fibrosis is colored blue. C group, control group; M group, monocrotaline group; PGE1 group, prostaglandin E1 group. *P<0.05 vs. C group, #P<0.05 vs. M group. Scale bars=150 µm (A–C), 50 µm (D–F). (G) Collagen content was greatly increased in the M group in comparison with the C group at 28 days. The PGE1 group showed a significant decrease in collagen content at 28 days.
|
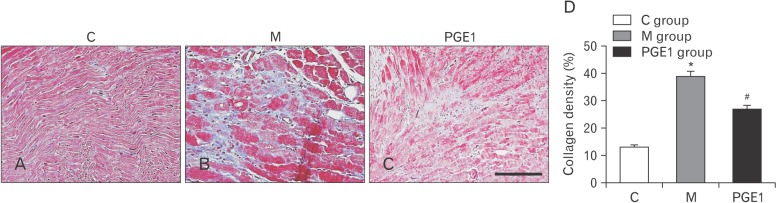 | Fig. 3Representative images of right ventricle stained with Masson Trichrome from C group (A), M group (B), and PGE1 group (C) at 28 days following the injection of monocrotaline. (D) Collagen content was greatly increased in the M group in comparison with the C group at 28 days. The PGE1 group showed a significant decrease in collagen content at 28 days. Fibrosis is colored blue. C group, control group; M group, monocrotaline group; PGE1 group, prostaglandin E1 group. *P<0.05 vs. C group, #P<0.05 vs. M group. Scale bar=150 µm (A–C).
|
Immunohistochemistry analysis of lung samples
Immunohistochemistry staining of lung tissues revealed that ET-1–positive cells were more prevalent in the PGE1 group, followed by those in the M group in comparison with those in the C group at 28 days (Fig. 4A-F). Three weeks after PGE1 treatment, ET-1–positive cells were still observed at the lung area in the PGE1 group. The increased level of ET-1 immunoreactivity observed in the M group was statistically significant (P<0.05). The decreased level of ET-1–immunoreactivity was also significant in the PEG1 group compared to the M group (Fig. 4G).
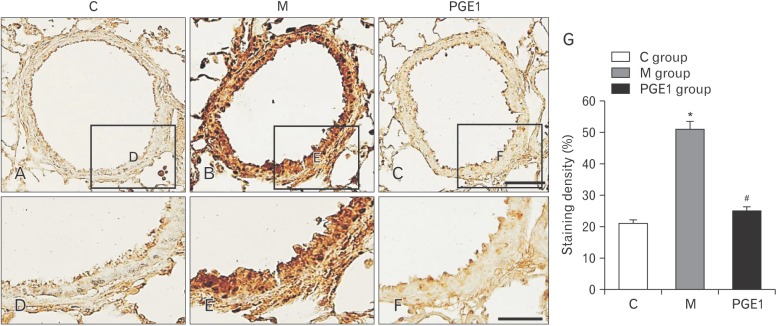 | Fig. 4Localization of ET-1–immunoreactive cells in the lung tissues at 28 days (A–F). Immunohistochemical expression reveals that the positive cells of ET-1 is significantly higher in the M group than that in the C group; however, it is lower in the PGE1 group than that in the M group (G). Panels (D), (E), and (F) are high power views of panels (A), (B), and (C). ET-1, endothelin-1; C group, control group; M group, monocrotaline group; PGE1 group, prostaglandin E1 group. *P<0.05 vs. C group, #P<0.05 vs. M group. Scale bars=50 µm (A–C), 25 µm (D–F).
|
TUNEL apoptosis assay
TUNEL staining was performed to detect apoptotic DNA in lung tissues. In the C group, there was no positive staining (Fig. 5A, D). However, the M group had lung tissues with positive TUNEL staining (the presence of dark brown nuclei was observed) (Fig. 5B, E). PGE1 group also had cells with brown nuclei, indicating apoptotic DNA (Fig. 5C, F). Apoptotic cells were significantly more prevalent in the M group than those in the C group. However, they were less prevalent in the PGE1 group than those in the M group (Fig. 5G). These results indicated that PGE1 could attenuate apoptosis in the lung tissues of treated PAH rats.
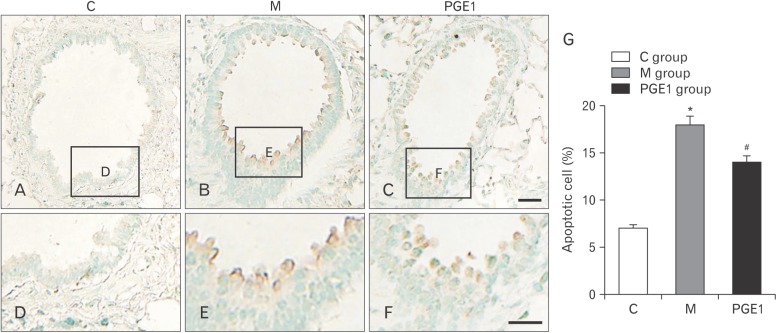 | Fig. 5TUNEL assay on lung tissues at 28 days after prostaglandin E1 transfusion (A–F). Immunohistochemical expression revealed that the positive cells of apoptosis were significantly higher in the M group than that in the PGE1 group; however, they were lower in the PGE1 group than that in the M group (G). Panels (D), (E), and (F) are high power views of panels (A), (B), and (C). *P<0.05 compared with the C group, #P<0.05 compared with the M group. TUNEL, terminal deoxynucleotidyl transferase-mediated deoxyuridine triphosphate nick-end labeling technique; C group, control group; M group, monocrotaline group; PGE1 group, prostaglandin E1 group. Scale bars=40 µm (A–C), 20 µm (D–F).
|
Western blot analysis
This experiment was designed to investigate if PGE1 group exhibited alterations in expression levels of ET-1 and ERA proteins in the lung. Changes in expression levels of ET-1 immunoreactivity in the lung were detected in the PGE1 group. Expression levels of ET-1 and ERA proteins detected in the PGE1 group were significantly decreased compared to those in the M group (Fig. 6A, B). Actin bands indicated protein loading in the same sample (P<0.001 vs. C group, P<0.001 vs. M group) (Fig. 6).
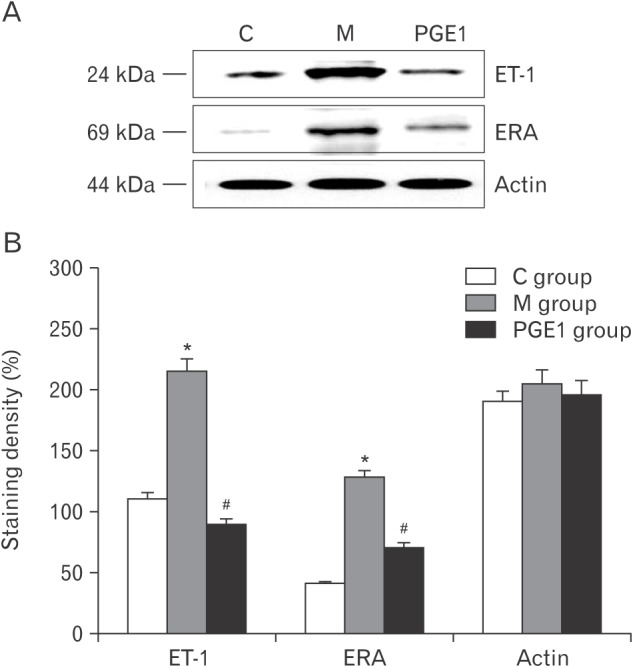 | Fig. 6(A) Western blot analysis of the levels of expression of ET-1, ERA, and actin immunoreactivity in the RV. (B) The semi-quantitative analysis confirms that PGE1 group exhibited increased levels of immunoreactivity of ET-1 and ERA in the RV. ET-1, endothelin-1; ERA, endothelin receptor antagonist; RV, right ventricle; C group, control group; M group, monocrotaline group; PGE1 group, prostaglandin E1 group (n=4–5 per group). *P<0.05 vs. C group, #P<0.05 vs. M group.
|
Go to :
Discussion
The present study showed that treatment with PGE1 could reduce mal-adaptive structural remodeling of the lung and heart and prevent ventricular arrhythmias in MCT-induced PAH in rats. The main purpose of this study was to determine the effect of PGE1 on PAH using a rat model. Our results showed that PGE1 did reduce SPAP in PAH rats. It also improved RV hypertrophy, an indicator of RV pressure overload caused by elevated pulmonary artery pressure. In addition, it decreased the number of intra-acinar arteries and medial wall thickening in pulmonary arterioles, index of vascular remodeling.
Endothelins are potent vasoconstricting peptides that have proliferative and pro-inflammatory effects. Isoform ET-1 is a well-established mediator of pulmonary vascular homeostasis [24]. Among other subtypes of PAH, higher levels of ET-1 are predictive of severity and mortality. ERAs can improve clinical and hemodynamic parameters of PAH. Therefore, ERAs are mainstays of PAH therapy [252627]. The following is our hypotheses about the mechanisms of how PGE1 decreases medial wall thickening. PGE1 has vasodilatory, antiinflammatory, anti-aggregatory, and anti-proliferative effects through decreasing the expression of ET-1 in lung tissues. However, when PGE1 is intravenously administered, it is rapidly eliminated by the lungs. The half-life of intravenous PGE1 can be as short as 42 seconds. Therefore, the clearance of intravenous PGE1 is closely related to respiratory function and pulmonary blood flow. In animal models of acute or chronic pulmonary hypertension, inhaled PGE1 can increase ventricular contractility and reduce pulmonary arterial pressure [28]. Inhalation of a single 25 µg dose of aerosolized iloprost, a prostanoid analogue, is associated with enhanced cardiac index and reduced mean pulmonary arterial pressure and pulmonary vascular resistance [29]. In previous studies, inhalation of 300 µg/day of PGE1 for 10 days following surgery is associated with reduced pulmonary arterial pressure, similar to the effect of intravenous PGE1 infusion [28]. Cortical hyperostosis of long bones is also reversible in neonates receiving PGE1 greater than 120 hours [30]. Therefore, the aim of this study was to evaluate the effect of continuous intravenous PGE1 on hemodynamics and long-term outcomes of rats with MCT-induced PAH. In the present study, we treated PAH rats with PGE1. We then performed hematoxylin and eosin staining, Masson Trichrome staining, immunohistochemical staining, and western blot analysis in order to investigate changes of ET-1 immunoreactivity in the cardiometer of these rats. A significant increase in pulmonary arterial pressure following MCT injection was accompanied by RV hypertrophy and increased lung and heart fibrosis when compared to the control group (Figs. 2, 3). In the RV of rats with PAH, PGE1 treatment decreased the development of RV hypertrophy and normalized the expression of collagen content (Fig. 3). Additionally, in rats with PAH, SPAP of the heart was decreased by PGE1 treatment (Table 1). There results suggest that PGE1 could decrease pulmonary vessel contraction and remodeling, leading to improvement in apoptosis and inhibition of fibrosis in PAH rats. These findings support our hypothesis that chronic PGE1 administration can improve PAH.
PGE1, a naturally occurring eicosanoid, is synthesized from 20-carbon polyunsaturated fatty acid dihomo-gamma-linolenic acid (DGLA) via cyclooxygenase-1 and -2 pathways [3132]. PGE1 is a member of series-1 prostaglandin class. It can produce a number of physiological effects. It is primarily known for its anti-inflammatory and vasodilatory effects. It has been reported that PEG1 can inhibit platelet aggregation, vascular smooth muscle proliferation, and collagenase activity [333435]. In pulmonary circulation, PGE1 is synthesized primarily by cells of the vascular endothelium and smooth muscle cells. Following intravenous administration, PGE1 is distributed and metabolized with an estimated half-life of 5–10 minutes [36]. Lungs are the primary sites for the metabolism of PGE1. They can metabolize as much as 80% of systemically absorbed PGE1 in a single pass [36]. Metabolism in pulmonary vascular bed is an oxygen-dependent process [37]. Prostaglandins including PGE1 are normally paracrine lipidic mediators. They can interact with a distinct family of G-protein coupled prostanoids receptors composed of 8 subtypes (EP1-4, IP, FP, TP, and DP) [38]. Of these eight subtypes, EP2, EP4, DP, and IP can induce smooth muscle relaxation and vasodilatory effects [39]. This mechanism is different from cardiac striated muscles where the troponin complex is responsible for the regulation of muscle contractions. PGE1 is also considered as a potential treatment option for PAH because of its high pulmonary clearance (70%–90%) and pulmonary-selective vasodilating effect [40]. However, intravenous administration of PGE1 has side-effects such as systemic hypotension and low cardiac output, similar to those produced by other short-acting prostacyclin analogues [40]. Recently, Della Rocca et al. [11] have documented the efficacy of inhaled PGE1 in improving pulmonary hemodynamics and oxygenation in a clinical trial enrolling 18 patients undergoing lung transplantation. They reported that PGE1 administered at a low dose produced a reduction in pulmonary arterial pressure and improved oxygenation without impairing systemic hemodynamics [11]. Thus, there is compelling evidence showing that PGE1 is a pulmonary-selective vasodilator that can be used as an alternative to current therapy for PAH. However, no study has attempted to develop a long acting PGE1. PGE1 might be used to treat cardiovascular disease. It has potential to induce vessel relaxation and inhibit excessive proliferation of vascular cells.
In conclusion, PGE1 can suppress PAH. Furthermore, PGE1 might be a new medicine for PAH. Further studies are needed to determine what pathways are involved in the improvement of PAH caused by PGE1.
Go to :