

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The omohyoid muscle typically has an inferior belly originating from the superior border of the scapula, near the suprascapular notch, and occasionally, from the superior transverse scapular ligament [1]. This muscle then passes deep to the sternocleidomastoid where its superior belly passes almost vertically upward next to the lateral border of sternohyoid to attach to the inferior border of the body of the hyoid bone lateral to the insertion of sternohyoid [2]. Reported variants of the omohyoid muscle include absence of its superior belly, duplicated superior belly, coursing deep to the internal jugular vein, and existence as the variant cleido-hyoideus muscle [3].
As the omohyoid muscle is commonly used as a surgical landmark during neck dissections (e.g., identified as the surgical landmark for level III and IV lymph node metastases), knowledge of its variations is important to surgeons. Herein, we report an unusual variant of the omohyoid and sternohyoid muscles.
Go to : 
Case Report
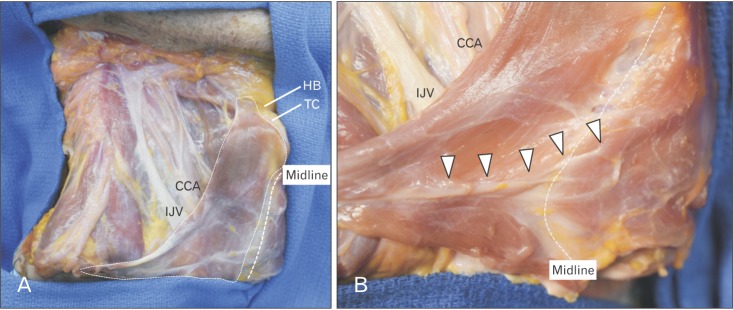
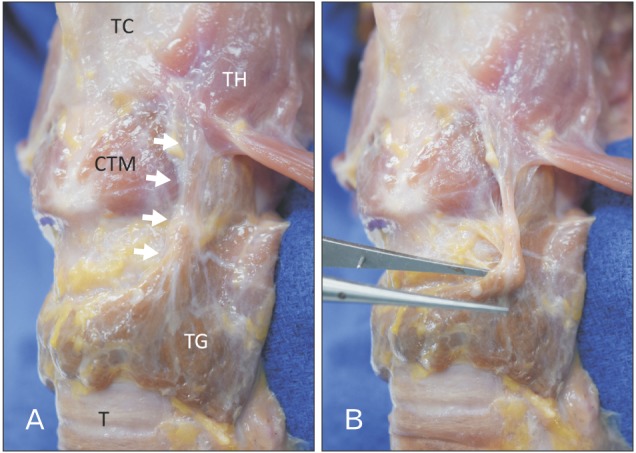
During the routine dissection of the neck in a fresh frozen cadaver head, fusion of the omohyoid and sternohyoid muscles into a single large sheet was found on the right side. The specimen was a Caucasian male cadaver whose age at death was 86 years old. The neck had been cut horizontally at the seventh cervical vertebra, so the inferior belly of the omohyoid muscle and attachment to the sternum of the sternohyoid muscle could not be observed. This large conjoined muscle was deep to the pretracheal fascia and ascended to attach onto the hyoid bone and thyroid cartilage (Fig. 1A). Two white tendons were found at the inferolateral part of this muscle; the superior tendon represented the intermediate tendon of the omohyoid muscle and the inferior tendon and traveled anteriorly to cross the midline and attach onto the left sternohyoid muscle (Fig. 1B). The muscle was innervated by branches of the cervical plexus and the ansa cervicalis was not observed. Deep to this abnormal muscle, the sternothyroid and thyrohyoid muscles were found and were normal in their morphology. The lateral edge of this fused infrahyoid muscle crossed the carotid sheath and its contents. On the left side, the infrahyoid muscles were normal, However, a slip from a left levator glandulae thyroidea muscle ascended and attached to the surface of the thyrohyoid muscle (Fig. 2).
As a cadaveric examination, the present study did not require approval by an ethics committee at our institutions, and the work was performed in accordance with the requirements of the Declaration of Helsinki (64th WMA General Assembly, Fortaleza, Brazil, October 2013).
Go to :
Discussion
In some studies, a doubled or duplicated superior belly of the omohyoid muscle has been reported [4]. In these reports, the inferior head of the superior belly of the omohyoid muscle was described as it fused to the sternohyoid muscle. Wood [5] reported duplication and triplication of the superior belly of this muscle and insertion onto the thyroid cartilage. The region between the sternohyoid and omohyoid has been reported to be filled with muscle slips instead of fascia [6]. However, no reports have shown the massive fusion between the omohyoid and sternohyoid muscles like the present case.
Embryologically, Loth [7] considered the omohyoid muscle to be a remnant of the sternocleido-omohyoid muscle, which consists of two layers, a sternocleidohyoid portion and an omohyoid portion. Buntine [8] described this primitive sheet of the muscle as the episterno-cleido-hyoideus or sterno- omo-hyoid. Unfortunately, in the present case, the inferior part of the muscle could not be observed due to prior dissection. However, we speculate that this sheet might represent the sternocleido-omohyoid muscle, which had not undergone atrophy.
The omohyoid muscle is used as a landmark to identify levels III and IV lymph node metastases of head and neck cancers [9] with the lateral border of the sternohyoid muscle defined as the anterior boundary of levels III and IV. In terms of surgical neck dissection, fusion such as reported in our case might mislead the surgeon and confuse the level classification of metastasis and thus alter postoperative therapy and prognosis by altering the anatomical landmarks used to localize lymph nodes in the region [10].
The omohyoid muscle is an important landmark for head and neck cancer treatment. Therefore, surgeons should be aware of its variations such as the one described in the current report.
Go to :
 XML Download
XML Download