

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The infraorbital foramen (IOF) is one of the most important facial foramina [1], and is located on the anterior face of the body of the maxilla [2], around 1 cm below the infraorbital border (IOB) [3]. The infraorbital artery and nerve [4], which are responsible for the vascular-nervous supply to important areas of the face [1], pass through the IOF.
It is important for surgeons and anesthetists to be aware of the possibility that anatomical variations may occur in the region of the IOF, when surgical interventions at the level of the middle third of the face or regional block of the infraorbital nerve are performed [567]. Thus, for good surgical practice, it is fundamentally important to have knowledge of the topographical anatomy of the facial foramina, such as the IOF [8]. The present work consisted of a morphometric study on the IOF, correlating this with sex and side of the cranium.
Materials and Methods
This morphometric study on the IOFs was conducted on dry human skulls that belong to the anatomy laboratories of the Federal University of Sergipe (UFS). Among the 242 crania examined, 148 were male and 94 were female, with and age range from 18 to 91 years. Crania that did not present any type of damage or bone alteration that might compromise the analysis were included in this study.
Measurements on the height and width of the IOFs (Fig. 1A) and the distances from the foramen to the IOB and anterior nasal spine (ANS) (Fig. 1B) were made with the aid of digital calipers with precision to 0.01 mm. Presence of foramina and their multiplicity was also observed. The center of the foramen was taken as the reference point, and distances were measured from this point. In cases of multiple foramina, the reference point was taken to be on the largest foramen.
The data were evaluated descriptively and analytically. The numerical variables were examined using the Shapiro-Wilk test to ascertain whether they presented normal distribution. In the cases in which the assumptions were met, the data were presented as means and standard deviations. If not, medians and interquartile ranges (25th to 75th percentile) were used. Categorical variables were presented as absolute and relative frequencies.
To compare the morphometric values according to sex, the Mann-Whitney test was applied. To compare between the sides, the Wilcoxon test was applied. The statistical significance level was stipulated as 5% (P≤0.05). For all the analyses, the SPSS version 15.0 (SPSS Inc., Chicago, IL, USA) was used.
Results
The ages of the 242 crania did not present abnormality and therefore were presented using the median. The general median was 57 years (range, 41.75–70 years). Among the male crania, the median was 57 years (range, 41.50–70 years), while among the female crania it was 56.50 years (range, 41.50–70 years). There was no statistical difference between these ages (P=0.887).
The IOF was present on both sides of the maxilla in all the crania studied, and in some crania, the presence of multiple IOF was observed. On the right side of the maxilla, 14 crania presented two foramina. On the left side, there were nine crania with two foramina; three crania with three foramina; and one cranium with four foramina. The associations between multiplicity of IOFs and sex are presented in Tables 1 and 2.
Occurrences of multiplicity (two foramina) on the right side of the cranium were more frequent in males: 78.6% (95% confidence interval [CI], 52.41–92.43), but there was no statistically significant association (P=0.168) (Table 1).
On the left side, presence of multiplicity consisting of two foramina was also more prevalent in males: 66.7% (95% CI, 35.42–87.94). All occurrences of three and four foramina were found in male crania. However, there was no association between multiplicity and sex (P=0.127) (Table 2).
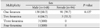
In comparing the morphometric variables between the sexes, statistical differences were found for the distance from the IOF to the ANS on both sides (P<0.001), and larger measurements were found in males. There were statistical differences in the height (P=0.007) and width (P=0.008) of the left IOFs, respectively, and in the width (P=0.004) of the right side, all in males (Table 3).
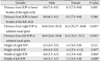
In comparing the morphometric variables between the right and left sides of the cranium, only the width of the IOF did not present any statistical difference (P=0.514) (Table 4).
Discussion
Knowledge of the characteristics and anatomical variations of the IOF may contribute towards reducing the risk of injury and sequelae of the infraorbital neurovascular plexus during surgical or anesthetic procedures. Injury to this neurovascular plexus may lead to profuse bleeding and/or numbness of the lower eyelid, ala of the nose, upper lip (including skin, mucosa, and gingiva) and upper incisors and canines [35910111213].
The frequency of multiplicity of the IOF has been found to range from 4% to 11% [3914]. In our study, multiplicity of the IOF was found in 10.7% of the crania studied, without any significant difference in relation to sex or the sides of the maxilla.
Regarding the distance from the IOF to the IOB too, we did not find any significant difference in relation to sex or the sides of the maxilla. Ekambaram et al. [14] reported that this distance was significantly greater on the right side, only in male crania. On the other hand, according to Macedo et al. [11], the distance from the IOF to the IOB was greater on the left side. In a study conducted in Brazil, Lira Júnior et al. [15] reported that the mean distance was 5.7 mm, while Saini [16] reported a distance of 6.7 mm. Both of those measurements were smaller than what was found in the present study, which was 8 mm. Although Ukoha et al. [17] did not make any comparison of the IOF between the sexes, they reported that in Nigerian crania, this foramen was significantly closer to the IOB on the right side than on the left side. Apinhasmit et al. [18] and Gour et al. [3] found means of 9.53 mm and 5.92 mm, respectively, for the distance from the IOF to the IOB, with significantly greater measurements in males. Rossi et al. [19] to evaluate the occurrence of craniofacial asymmetries in four distances it was shown that asymmetry of facial bones exists in fetuses and newborn with the same index as adults. Russo and Smith [20] sowed the presence of asymmetry in the skull base. This study demonstrated that the skulls in all age groups presented asymmetry and that in most of the measures there was prevalence of the right side over the left side.
The values found for the distance from the IOF to the ANS in our study varied significantly between the sexes and between the sides of the maxilla. These findings were very similar to those described by Ekambaram et al. [14] and Lopes et al. [10]. However, the mean values found for this variable in the study of Ukoha et al. [17] were smaller, which may be associated with anatomical differences between different ethnic groups. However, Przygocka et al. [21] has drawn attention to the fact that parameters used to locate the IOF should be applied with great caution when evaluating patients from different populations. These authors also point out that studies originating from Europe, Asia, Africa, and North and South Americas are difficult or even impossible in some situations as the measurements were often taken in different ways.
Joseph et al. [9] found statistically significant differences in the height and width of the IOF in relation to sex, such that these were larger in male crania. In our study, only the height of the IOF on the right side did not present any statistically significant difference. For the height of the IOF on the left side, and for the width of the IOF on both sides of the maxilla, the measurements were statistically greater in males. The mean values for the height and width of the IOFs found in our study were similar to those found by Joseph et al. [9] and Saini [16], but were slightly smaller than those described by Boopathi et al. [22]. Moss and Greenberg [23] in the functional analysis performed on the maxillary bone showed that the occurrence of variation in the width and length of the IOF was dependent on the type of dentition. The authors have highlighted three points from the IOF: the increase of the foramen on posterior direction when the downward, forward, and lateral growth, of the maxillary bone; the IOF is a fixed point of reference to the other maxillary structures; and a relation between the orientation of the IOF with changes in the maxillary bone growth. Schwartz [24] also justified the variability of the IOF with the embryological development of the upper jaw and the dentition.
The IOF was present in 100% of the samples, on both sides of the maxilla, and the rate of occurrence of multiple foramina was 10.7%. Only one cranium presented multiple foramina bilaterally. There was no association between this variable and sex. The mean distance from the IOF to the IOB was 8 mm, without any difference between the sexes, but it was significantly greater on the right side of the cranium. The mean distance from the IOF to the ANS was 36 mm in males and 34 mm in females, with a statistically significant difference between the sexes. The mean heights and widths of the left and right IOFs were 4 mm. The height of the IOF was significantly greater on the right side. The width of the IOF was significantly greater in males.



 XML Download
XML Download