

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Mandibular ramus has two processes (coronoid and condylar). The coronoid process projects upwards and slightly forwards as a triangular plate of bone. Its posterior border bounds the mandibular notch and its anterior border continues with mandibular ramus [1]. Although the coronoid process is not part of the temporomandibular joint, its hyperplasia or elongation can effect the mandibular movement [2]. The elongation of coronoid process of mandible is rare condition characterized by abnormal bone development which cause malocclusion or facial asymmetry and the limited mouth opening which was responsible to oral hygiene failure and pain [3456]. In this condition, coronoid process consists of histologically normal bone [6]. It leads to impingement of the coronoid process on the body or arch of the zygomatic bone on opening of the mouth [57].
This condition was firstly described by Lagenbeck in 1853 and a similar problem which was characterized by a synovial pseudoarticulation between zygoma and hyperplastic coronoid process was described by Jacob in 1899 [8]. It was seen in a large range of age from 3 to 78 [6] but was often in the 2nd–3rd decade [468]. The aetiology of the hyperplasia is not clear. Trauma, endocrine stimulus, hyperactivity of the masticatory muscles, pathological muscle tissue, heredity were suspected [569101112]. This study displays a new variant of bilateral elongation of coronoid process with different presentations in an Anatolian skull.
Case Report
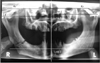
The present case of elongation of the coronoid process was obtained as an incidental finding in adult skull from the Department of Anatomy, Medical Faculty, Ondokuz Mayıs University, Turkey. The coronoid processes of this mandible bilaterally, seen so longer than normal. We used panographic analysis for the bilateral case and took photographs (Figs. 1, 2). All of the measurements were taken by using a digital caliper. The length of coronoid was measured as distance between tip of the coronoid process and mandibular notch. The lengths of coronoid processes were 2.5 cm and 2 cm for right and left sides, respectively. The right coronoid process extended about 1.6 cm above the inferior rim of zygomatic arch. It was 1 cm for left coronoid process.
In our case, Levandoski panographic analysis [13] was performed on the panoramic radiographie to determine the elongation or hyperplasia of the coronoid process. We made a reconstruction with the dry mandible and a skull in the aim of taking the panoramic radiography to which we planned to apply the Levandoski panographic analysis. The mandible was articulated with the skull by the condylar process. To obtain the original teeth distance between mandible and maxilla on the front view, which was occured by the absence of teeth, we used a cotton tamponade which has average 15 mm thickness, than after we took the panoramic radiography (Fig. 3).
To perform the Levandoski panographic analysis [13], three reference points were taken condylion (Cd), gonion (Go) and koronion (Kr) and marked on the radiogram. After that, four lines were taken as follows: line 1, the maxillary vertical midline passing through the nasal septum; lines 2-3-4, perpendicular to the line 1, passing through the lower border of the mandibular symphysis, tip of the condyle and the tip of the coronoid process, respectively (Fig. 3). The measurements were taken from the tip of the condylar process and the tip of the condyle to the mandibular symphyseal line at vertical direction and the ratio of these two measurements (Kr-Go/Cd-Go) were obtained. The right condylar process was exactly hyperplastic. The measurements of Kr-Go/Cd-Go were 95.10 mm/79.03 mm on right side and 97.53 mm/87.80 mm on left side. The ratio of Kr-Go/Cd-Go on the right side was 1.20. The other bones of skull were normal.
Discussion
The elongation of the coronoid process was a rare condition that leads to restricted mouth opening.It was previously evaluated using magnetic resonance (MR) and computed tomography (CT) imaging [581014]. It has been reported that 31 cases were recorded during a 20 year period from 1970 to 1990 at the Queen Victoria Hospital [6]. And also noted 40 bilateral and 5 unilateral cases which were previously reported by different investigators in a period of 1957 to 1994 [6]. Hönig et al. [2] performed an investigation on panoramic radiographies in order to access the prevelance of the asymptomatic enlargement of the coronoid process and found only one hyperplastic coronoid process. Mulder et al. [4] made a literature search from 1995 to 2010 and found 61 cases. Javid [15] reported a case which had an enlarged coronoid process protruding at least 1 cm over the inferior rim of the zygomatic arch. Also, it was bilaterally found by Munk and Helms [9] in two patients and unilaterally in one patient.
Pregarz et al. [5] reported the four bilateral cases and one unilateral case of elongation of coronoid process using MR, CT imaging, and panoramic radiographies. One of their bilateral cases showed the coronoid process of both side extented about 2 cm above zygomatic arch. In these cases, they detected slight facial asymmetry with flattening of the zygomatic arches and inpingement of the coronoid process on the zygomatic arches which showed the development of osteophytes. Ilguy et al. [12] observed bilateral three cases of elongation of coronoid process using cone beam CT. They used the line passing from the tip of the condyle that was parallel to the Frankfort plane for the vertical length of the coronoid process. In three cases, according to 3D view they found the length of coronoid process as 6.1 mm, 15.2 mm, and 8.3 mm on the right side and as 5.4 mm, 9.5 mm, and 6.1 mm on the left side, respectively.
Chauhan and Dixit [16] reported the length of the coronoid process of a dry mandible as 2.4 cm on the right side and 2.6 cm on the left side. Lucaya et al. [3] detected radiologically elongation of the right coronoid process which protruded more than one centimeter above the inferior rim of zygomatic arch and impinged on the posterior aspect of the malar bone in one case. Izumi et al. [14] investigated the temporomandibular joints of 1,665 patients using CT and found the incidence of elongation of the coronoid process as about 0.3% (4 cases).
In our case, coronoids project much above the level of condyles in the mandible of late adulthood. The ratio of Kr-Go/Cd-Go on the right side was higher than the Levandoski's [13] minimal 1.15 for hyperplasia. On the left side the ratio was 1.11. This was under the 1.15 but higher than the "1.07," that the Levandoski's [13] maximal ratio for the normal coronoid process. On the other hand, at the photographs, the tip of coronoid process was seen over the zygomatic arch. The most of authors noted that if the coronoid process passes over the zygomatic arch, it mostly cause restricted jaw movement, so the coronoid process was hyperplastic [591114]. We could say that, according to the Levandoski panographic analysis, the ratio of the left coronoid process was higher than normal but not over the minimal ratio for hyperplasia.
In the aetiology of the coronoid hyperplasia trauma, endocrine stimulus, hyperactivity of the masticatory muscles, pathological muscle tissue, heredity were suspected [569101112]. El-labban et al. [17] reported the occurrence of amianthoid fibres, which were thick collagen fibres that can be 1,000 nm in diameter, in the temporalis muscle in the coronoid hyperplasia patients by electron microscopy. Pregarz et al. [5] noted the hypertrophy of the tendinous insertion of the temporalis muscle in one patient.
Development of the lower jaw occurs mainly between fourth and eighth weeks of gestation, from paired mandibular primordia (mandibular prominences). In the fourth week of gestation, proliferation of neural crest cells that migrate into the branchial arches produce the mandibular prominences. The neural crest cells come from the region of the hindbrain and give rise to cartilage, bone and ligaments in the facial and oral regions [18].
In the fifth week of fertilization, a pair of Meckel cartilage appears and in the sixth week, the mandibular ossification begins. In seventh week, the lineer trabeculae of mandible, which will be branched toward the future mandibular symphysis, alveolar bone, mandibular body and coronoid process, developed. At this time the primordial masticatory muscles (masseter, temporalis, and pterygoid) were located around the Meckel's cartilage. In ninth week, temporalis muscle attached to the coronoid process. In 10th week, the mandibular ossification advanced to form the mandibular angle, coronoid process and symphysis. From week 12 intramembranous ossification was active at mandibular body, coronoid process and symphysis [19]. Because of their immaturity, the masticatory muscles do not effect on the early embryonic mandibular movement but the fetal age of 11 weeks is important for jaw development; the action of masseter and temporalis muscles interacts with ramus growth at this stage [20].
The variations in the number, mitotical activation and the rate of division of stemcells can effect ontogenetic and phylogenetic modification of mandibular morphology [21]. The hyperactivity of the temporal muscle and evolutionary change in the mandibular morphology can cause elongation of coronoid process [212223]. To our knowledge, the elongated coronoid process of skull that was determined, using Levandoski panoramic analysis has not been reported yet. Elongated coronoid process is one of the factors cause mandibular hypomobility [24], it as reported here might lead to limited mouth opening. The knowledge of this variation or abnormality can be useful for the radiologist and surgeons and prevent misdiagnosis.


 XML Download
XML Download