

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Foot pain is a very common symptom in patients with orthopaedic problems. Additionally, people who enjoyed various outdoor activities have increasingly experienced foot pain in the recent past [1]. Most foot pain is caused by entrapment of the tibial nerve and/or its branches in the ankle [234]. The most common causes of entrapment of nerves can be broadly classified into three types: trauma, spaceoccupying lesions, and deformities of the foot [25678]. The symptoms include burning pain, numbness, paresthesia in the toes and sole of the foot, occasionally pain that radiates upwards on the medial side of the calf [25891011]. Treatment of foot pain, caused by entrapment of nerves in the ankle, involves injections and operations. Some authors have reported a need for anatomical knowledge of neurovascular structures in the ankle region to diagnose and treat foot pain [56712].
Studies to date have described about the tibial nerve and its branches [910131415]. Textbooks have individually addressed the posterior tibial artery and the tibial nerve, but have not described the relationship and location between the artery and nerve. In this study, we classified the relationship between the tibial nerve and the posterior tibial artery and marked bifurcations of neurovascular structures in the ankle region using anatomical landmarks to map out areas. We have thus determined the location of neurovascular structures and accordingly suggested the safe zone for treatment, in detail.
Materials and Methods
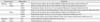
Ninety feet, 41 male feet and 49 female feet, of embalmed human cadavers were examined. There were a total of 43 right feet and 47 left feet. The average age of cadavers was 70 years (range, 46-96 years). After the removal of skin and fat from the foot and ankle, 3 bony landmarks were marked at the inferior tip of the medial malleolus of the tibia (M), the posterior superior tip of the calcaneal tuberosity (C), and the medial process of the calcaneal tuberosity (P) (Fig. 1). Based on the strategy of classification and measurements, a line between the medial malleolus of the tibia (M) and the posterior superior tip of the calcaneal tuberosity (C) was set as a reference line (Line A).
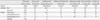
Primarily, the neurovascular structure in human ankle region was classified by the following criteria: (1) the relationship between the posterior tibial artery and the tibial nerve; (2) the anatomical position. Lastly, bony landmarks and neurovascular structures were examined from 9 measurements. The details of measurements were as follows: 1 distance between the bony landmarks and 8 variables in arteries and nerves, respectively. There were 7 distances, 1 external diameter, and 1 width (Table 1). In addition to the measurements, we noted a number and origin of the medial calcaneal branches of the posterior tibial artery and the tibial nerve. Line A was set to zero for the purpose of measurements and if the bifurcation of artery and nerve was located distal to Line A, it was designated with a negative number. The neurovascular structures were expressed as a ratio of the location to distance between the bony landmarks M and C (DMC). The locations of bifurcated neurovascular structures were particularly noted as X- and Y-coordinates. X-axis was the reference line in this study and Y-axis was a line perpendicular to the X-axis. An ankle angle might affect values of distance dimension so it was adjusted and fixed by a right angle during the measurement.
The data were statistically processed descriptive statistics, independent t-test, paired t test, and chi-square using the computer program (version 17.0, SPSS Inc., Chicago, IL, USA).
Results
Four amongst 9 measurements did not exhibit statistically significant difference between males and females. In a numerical value, the location of the artery and nerve at Line A showed a statistically significant difference between the sexes (P<0.05), the tibial nerve at Line A was marked no significant difference between the sexes in the ratio (Tables 2, 3). Approximately 60% of the lateral plantar nerve headed toward the direction of the medial plantar nerve and the proportion was similar in both sexes.
Classification
The most common type of relationship between the posterior tibial artery and the tibial nerve was type I (50 feet, 55.6%), where the posterior tibial artery was located medial to the tibial nerve. Type III was the least common type (3 feet, 3.3%), wherein the posterior tibial artery was located lateral to the tibial nerve. Type IV, in which the tibial nerve was already separated proximal to Line A was prevalent in 16 feet (17.8%). Table 4 displayed the classification of the relationship between the posterior tibial artery and the tibial nerve. The classification showed statistically significant difference between both the sexes (χ2=52.489, P<0.01) (Fig. 2).
Tibial nerve
The tibial nerve was bifurcated to the medial and lateral plantar nerve after passing at Line A in 82.2%. The tibial nerve at Line A, passed by around 3 cm from M and divided into the medial and lateral plantar nerves at approximately -0.5 cm perpendicularly from Line A. The tibial nerve located around 45% with DMC (distance between the bony landmarks the tip of the medial malleolus of the tibia and the posterior superior tip of the calcaneal tuberosity) at Line A. The bifurcation of the tibial nerve was more proximal than Line A in 24 feet (26.7%), and it diverged from the same positions as Line A in one foot (1.1%). The most proximal location of the bifurcation was around 5 cm from Line A. The tibial nerve was located proximal the Line A in 41.5% of males and 36.7% of females. The average location of the bifurcation was at 48% in X-coordinate and -10% in Y-coordinate (Table 3). The location of the tibial nerve in males was not significantly different from that in females.
Posterior tibial artery
All posterior tibial arteries were separated to the medial and lateral plantar arteries after passing at Line A. The posterior tibial artery was located around 3 cm from M at Line A. Its bifurcation was perpendicularly -2 cm away from Line A, and -3 cm from M. The location of the posterior tibial artery at Line A showed statistically significant difference between both sexes (P<0.05). Although the posterior tibial artery was located close to the tibial nerve in both the sexes, the location was statistically significant difference between the posterior tibial artery and the tibial nerve at Line A (P<0.01). The entire posterior tibial artery was divided more distal to Line A. The posterior tibial artery passed around 48% at Line A, and divided on an average at 41% and -38% in X- and Y-coordinates, respectively (Table 3). X-coordinate of the posterior tibial artery was statistically significant difference between males and females.
Calcaneal branches
The medial calcaneal branch of the posterior tibial artery mostly originated in the lateral plantar artery (43.3%) and had only one branch (56.7%). Generally, the medial calcaneal branch of the tibial nerve originated from the tibial and lateral plantar nerves simultaneously (55.6%) and had two branches (42.3%) in this study. One foot had 5 medial calcaneal branches of the tibial nerve. The number and origination of the calcaneal branches in males were similar with in females statistically (Table 5).
Discussion
Neurovascular structures observed in the ankle region were different between sexes and amongst individuals. The location of neurovascular structures were expressed as DMC and the bifurcation of neurovascular structures was expressed in X- and Y-coordinates in this study. The tibial nerve was initially at around 50% of DMC, and soon coursed towards the heel; it subsequently divided into the medial and lateral plantar nerves. The posterior tibial artery was numerically located posterior to the tibial nerve at Line A, but soon crossed anterior to it in both sexes (Table 3). The posterior tibial artery was located on 48% at Line A and then on 41% at the bifurcation point. The tibial nerve was showed around 45% at Line A, 48% at the bifurcation point. According to a report by Gamie et al. [16], X-coordinates in the artery and nerve were located as almost 60% at Line A. This difference was statistically significant (P<0.01) (Table 6).
The bifurcation of the tibial nerve has been reported using the standard line [91314], but the bifurcation of the artery was not described in detail. Dellon and Mackinnon [14] reported that the bifurcation was at the standard line (55%) and that the majority of it was within 2 cm of the standard line (94%). Havel et al. [9] declared that the bifurcation occurred at the standard line in 26 feet (38%) and within 2 cm in 63 feet (93%). Most of the bifurcations were distributed at -1 to -1.9 cm according to the Bareither et al. [13] study (27%). However in this study, the location was -2 to -2.9 cm (50%) from the distal to the tip of medial malleolus. It was difficult to compare the bifurcation between the standard lines amongst the studies. However, the bifurcations in Bareither et al. [13] and this study were located more proximal side than reported by Dellon and Mackinnon [14] and Havel et al. [9] (Fig. 3). Thus, the locations to be considered during diagnosis and treatments differ among population groups.
The bifurcations of the tibial nerve and the posterior tibial artery were represented by the distribution using territories, based on the central point of bifurcations, as follows 25%, 50%, and 75%, respectively (Fig. 4). The territories of the posterior tibial artery were similar to in males and females. The range of X-coordinates of the posterior tibial artery was 30% to 56%, and of Y-coordinate was -26% to -50% in males; whereas, the range of X-coordinates was from 27% to 51% and the Y-coordinate was -28% to -52% in females. Contrarily, the territories in the tibial nerve were formed both up and down in a longer and narrower shape in males than in females. The range of X-coordinate was 39% to 57% and of Y-coordinate was from -45% to 36% in males; while the range in females was 29% to 65% in X-coordinate and -10% to 39% in Y-coordinate.
The nerve branching patterns of the medial calcaneal branch were slightly different among the studies (Table 7) [91417181920]. Previous and this studies reported that multiple branches were most common. Rondhuis and Huson [20] described all samples with one medial calcaneal branch, and Andreasen Struijk et al. [18] reported that half of the samples had one branch while the other half had several branches. Govsa et al. [17] and this studies mentioned and counted the 'multiple' origin. Thus, the medial calcaneal branch originated from the tibial nerve and the lateral or medial plantar nerves simultaneously [17]. Rondhuis and Huson [20] described the origin of the medial calcaneal branch from the tibial nerve, in all samples. Whereas five others studies reported that the origin of the medial calcaneal branch in most samples was from the tibial nerve [914181920]. Unlike these studies, some authors [91819] have reported that the origin of the medial calcaneal branch was the medial plantar nerve.
Foot pain due to an entrapment neuropathy is not easy to diagnose and treat. The diagnostic methods have been recommended for the definite diagnosis of peripheral nerve entrapment, such as tarsal tunnel syndrome: history, physical examination, radiological, and electrodiagnostic studies [21]. Diagnosis can be made by any combination of prolonged motor and sensory conduction velocity of the tibial nerve and its branches, because studies on conduction velocity generally fail to provide localizing data from a single nerve tract examination [7]. Treatment of an entrapment neuropathy involves physical therapy, injection, and operations. Kim et al. [22] involves dissection of the flexor retinaculum and connective tissue around the neurovascular bundle of the tibial nerve and vessels due to less incision. They announced that is useful because postoperative management does not require immobilization and patients can walk immediately and resume to their normal lives [22]. As noted in the above, to the successful diagnosis and treatment, it is important to know the detailed anatomy of the neurovascular structure at ankle region. In this study, the location of the artery and nerve were showed statistically significant difference between males and females in the numerical value, but the location of the tibial nerve in males was not differed from in females in the ratio. Therefore, this study proposed a description of neurovascular structures in the human ankle region by the ratio, X- and Y-coordinates, and territories. We suggested that a danger zone was based on the territories of the neurovascular structures (Fig. 5). The neurovascular structure always located in this area. If surgeons approach this area you could be injured with the neurovascular structure, so this study named this area to 'danger zone'. The proposed methods were capable of overcoming the differences in size, and rendered a more accurate location of neurovascular structures. To diagnose, physical examiners look around 39% to 53% of a distance between the tip of the medial malleolus and the posterior superior tip of the calcaneal tuberosity. To treat, surgeons approach around 32% to 65% at a reference line and 13% to -39% perpendicular to a reference line. This study provided both, objective and precise information on the neurovascular structures based on the anatomical landmarks.










 XML Download
XML Download