

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The pes anserinus (PA) is composed of the combination of tendinous insertions of the sartorius, gracilis, and semitendinosus muscles. These three muscles attach to the medial side of tibia to generate a shape reminiscent of a goose's foot, which is the literal meaning of its name. This structure is clinically important in the reconstructive surgery involving tendons or in the steroid injection for anserine bursitis (AB).
The PA tendons are commonly used as autografts in ligamentous reconstruction of the knees [1, 2]. The main advantage of this approach is the low donor side morbidity and the fact that harvesting PA tendons does not lead to any clinical or functional deficits [1]. However, a minimally invasive surgery demands an understanding of the exact locations of PA tendons from the insertion site.
There have been anatomical studies investigating on the shapes of the PA in various populations [1, 2, 3]. The present study sought to determine in detail the relation between the relative positions and shapes of the insertion site and the PA, in a Korean population.
The anserine bursa is located at the upper medial aspect of the tibia, at the insertion of the conjoined tendon of the PA muscles. The AB can often be the source of discomfort in patients experiencing knee pain [4]. The AB has been clinically diagnosed in 46.8% of the patients with knee osteoarthritis. In contrast, 83.3% of AB or tendinitis patients were reported to have radiographic evidence of knee osteoarthritis [5].
Steroid injection in the bursa is a method to treat bursitis that can provide pain relief [4, 6, 7, 8, 9]. The accuracy of anserine bursa injection with ultrasound-guidance is markedly higher compared to the blind injection [10]. In clinical practices, however, surgeons are often confronted with the situations requiring blind injections, although they are well-aware that the ultrasound-guided injection is highly preferred. In the case of a blind injection, understanding and identifying the recommended site based on the anatomical knowledge would be very helpful.
Prior studies have investigated the human bursa [11, 12, 13, 14, 15, 16, 17, 18, 19], but the anatomical information of anserine bursa was limited. In this reason, The aim of this study was to identify the boundary of the anserine bursa to determine the recommended injection site and the shape of the insertion area of PA.
Materials and Methods
The present study aimed to investigate the shape of a footprint of the PA, 60 embalmed and 26 non-embalmed specimens from 45 Korean adult cadavers (26 males and 19 females, age range of 49-96 years, and height range of 150-178 cm). Each cadaver was placed in supine position and the knee joint was maintained at a 90° flexion before dissection. An incision was made at the knee area on the antero-medial surface. After removing the skin around the knee, the insertion site of the PA tendons was exposed completely and was carefully dissected to identify the shape of the PA. The width of the insertion site was measured and the shape of the insertion site was recorded with photographs and by drawing. Water was sprayed on the cadaver during dissection to prevent them from drying. The measurements of the PA were performed as follows (Figs. 1, 2, 3):
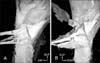
To investigate the anserine bursa, 34 non-embalmed specimens from 18 Korean adult cadavers (9 males and 9 females, same ranges in age and height as previously noted) were studied. Each cadaver was placed in supine position and the flexion of the knee joint was maintained at about 90°. The skin and soft tissue around the knee area were removed. To find the best injection site in the anserine bursa, various methods were explored in the preliminary study. The optimal location for injection, which was presently used for all specimens, was 20 mm medial from the IMPTT, with the superior border of sartorius from that point used as the injection site. A solution of 26 ml containing 5.0 g of gelatin (Merck, Darmstadt, Germany) and 3 drops of blue ink (Maepyo, Seoul, Korea) was injected into the bursa by using a 50 ml syringe with 20 gauge needle. The injection-needle was positioned at 20° from the vertical line medially and inferiorly, at the point of about 20 mm medial to superior border of sartorius from the IMPTT (Fig. 4). The nerves and vessels on the anserine bursa were traced to determine their distribution (Figs. 5, 6). After checking the shape of PA at the insertion site, the shape of bursa was determined and recorded as described above. The measurements of the anserine bursa are as follows:
A single observer made all measurements using a digitalized caliper (Absolute Digimetric, Mitutoyo Corp, Kanagawa, Japan). Also, we divided into 9 parts on the basis of maximum and minimum points on the bursa. Then, we investigated the frequency of the passage of vessels and nerves in each of the 9 parts for all specimens, and the frequency was presented in percentage (Fig. 6). All metric data were analyzed by using SPSS version 15.0 (SPSS Inc., Chicago, IL, USA). Comparisons between males and females were performed by using the t-test. P-values of < 0.05 were considered significant.
Results
The insertion width of the sartorius on the medial side of the tibia was 32 mm (range, 26.0 to 37.0 mm). The average tendon width was 7.0 mm (range, 4.0 to 10 mm) for the gracilis and 10 mm (range, 7.0 to 14 mm) for the semitendinosus at their tibial attachment site. The average width for the injection site of superior border of sartorius was 12±3.0 mm (minimum 6.0 mm, maximum 17 mm). No significant difference was observed between all variables in males and females (P≥0.05).
The sartorius tendon was inserted in the superficial layer, and the gracilis and semitendinosus were inserted deeper on the medial surface of tibia. In one specimen, some parts of sartorius tendon were inserted deeper than the gracilis and semitendinosus tendons (Fig. 1). When we designated the inferior borders of sartorius on the insertion site as a reference line, the semitendinosus was attached to the inner space of the inferior borders of sartorius in 70% of the time (60 specimens), while it was attached inferior to the sartorius in 30% of the time (26 specimens) (Fig. 2). The number of semitendinosus tendons at the insertion site varied: 1 in 66% of specimens, 2 in 31%, and 3 in 3% (Fig. 3). The semitendinosus tendons were usually connected to the deep fascia of the leg. It is fused with the periosteum over the subcutaneous surfaces of the bones.
Overall, the shape of anserine bursa was irregularly circular. Most of the anserine bursa in the specimens reached the proximal line of the tibia (about 65±7.0 mm from the IMPTT). The inferior border of anserine bursa was, on average, located at about 16 mm from the IMPTT. However, 8 out of 34 specimens had location at 20 mm above the proximal line of the tibia. In the medial view of the tibia, the anserine bursa was located posteriorly and superiorly from the tibia's midline, and it followed the lines of the sartorius muscle (Fig. 5).
When the bursa was divided into 9 parts, area C2 contained the largest number of nerves and vessels. Area A2 and A3, which corresponded to the injection point, contained only 6.4% (24 cases) of the nerves and vessels (Fig. 6).
Discussion
The present findings echo those of Laprade et al. [20] in American specimens, and show that the sartorius tendon fascia is intimately attached to the superficial fascial layer, whereas the gracilis and semitendinosus tendons are located in the deep surface of the superficial fascial layer over the medial aspect of the tibia. The average widths of the PA tendons in the previous and present studies differ by only 1.0 mm, indicating no influence of ethnicity.
Variations such as an accessory band of the gracilis and semitendinosus were frequent. Another study using 10 human cadaveric specimens reported that the accessory bands may arise from these two muscle tendons and insert separately into the PA [1]. The latter study [1] reported with dissections of accessory bands in all gracilis and semitendinosus tendons. These two muscles are also connected to the crural fascia, and the semitendinosus tendon was found with 31% of bifid tendons and 3% of trifid tendons (Fig. 3). In one specimen, the sartorius tendon was inserted in bifid form to the tibia (Fig. 1). Mores study in detail should prove many useful findings applicable to the reconstructive surgery.
Many cases involving pain in the PA insertion region are diagnosed as PA tendinitis or bursitis syndrome. The diagnosis is entirely based on clinical manifestations marked by spontaneous medial knee pain on climbing or descending stairs, tenderness at the PA insertion, and occasional local swelling [5]. The incidence of AB is higher in women; overweight individuals; individuals with osteoarthritis of the knees, valgus deformities, and pes planus; and those of 50-80 years of age, although younger obese women can also be affected [7, 9].
Presently, the proximal boundary of the anserine bursa was 10 mm medial from the IMPTT and the distal boundary continued in the postero-superior direction in relation to the tendons of PA (Fig. 6). The bursa of almost all specimens reached the proximal tibial line, but 8 of the specimens reached 20 mm above the line. These results may lead to further studies for useful understanding and treatment of AB.
Some of the present specimens displayed infrapatellar nerve near the bursa from the saphenous nerve and vein in the inferior direction. However, this was not related to the injection site, which was located 20 mm medially from the IMPTT. The anserine bursa was distributed widely, from the medial surface of the tibia, in the posterior direction on the gastrocnemius muscle area. The observations from this study support the proposal that when a surgeon performs an injection in the bursa, the injection should best be done on the medial surface of the tibia than away from it at the posterior part. This was explained by basing the choice of site at 20 mm medial to the IMPTT.
In conclusion, the results of this study recommend the injection method best performed with prevention of damaging the vessels and nerves. The injection for AB should be carried out at 20° from the vertical line medially and inferiorly, 15 or 20 mm deeply, and at the point of about 20 mm medial and 12 mm superior from IMPTT (Fig. 4).





 XML Download
XML Download