

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Numerous variations of human vascular patterning are possible in both peripheral circulation and large vessels including the aorta [1, 2]. Several anomalies of the aortic arch may occur depending on the site of involution of the embryonic aortic arches. These result from abnormal or incomplete regression of 1 of the 6 embryonic brachial arches [1, 2]. The arterial variation described here was identified during a dissection demonstration for students in the Department of Anatomy at the Chonbuk National University Medical School. Detection of these anomalies before any surgical intervention is important to determine the appropriate operative approach by either the open or endovascular route. The branching pattern of the aortic arch described in this study-a single aortic arch curving to the right instead of the left with the left common carotid, right common carotid, and left subclavian arteries as branches-is unique and has not been reported previously in a Korean subject.
Case Report
During a routine dissection course at the Department of Anatomy at the Chonbuk National University Medical School, a rare anatomical variation in the vessels of the aortic arch was observed. The cadaver, donated to the Department of Anatomy, was that of an 89-year-old Korean woman. The supracardiac arteries were removed from the female cadaver en bloc at autopsy. The arterial bloc included the ascending and proximal descending aorta with the branches of the aortic arch extending superiorly as far as the proximal external and internal carotid arteries and laterally beyond the origins of the vertebral arteries from the subclavian arteries. The bloc was fixed and stored in 10% formalin. Following fixation and gross examination, each branch of the aortic arch was divided at its origin. The external diameter of a 9-15-mm long arterial segment was measured and photographed using a dissecting microscope.
In this case, the ascending aorta arose from the left ventricle and ascended obliquely, curving forward and to the right, and became the aortic arch. The right-sided aortic arch first ascended and reached a summit at the T3 vertebral body level, and then curved dorsally along the right side of the trachea and the esophagus. The right thoracic aorta, a continuation of the aortic arch, descended to the right of the vertebral column (Fig. 1). This case did not present with situs inversus viscerum. The heart was of normal size and its relationship with the aorta and the pulmonary trunk was unremarkable. The lungs were also normal in size with no evidence of deformities.
The four branches originating independently from the anterior wall of the aortic arch, arranged in order from right to left, were the left common carotid, right common carotid, right subclavian, and retroesophageal left subclavian arteries (Fig. 2). After arising from the aortic arch, these arteries had fundamentally normal courses with no abnormal ramifications. Distal to the left subclavian artery branch, the aortic arch dilated and formed the aortic diverticulum posterior to the esophagus. The ligamentum arteriosum connected the left end of the aortic diverticulum and the left pulmonary artery near the left side of the trachea and the esophagus.
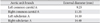
The external diameter of the left common carotid artery, located proximally on the aortic arch, was approximately 9.25 mm at its origin (Table 1). After arising from the left side of the anterior wall of the aortic arch, the left common carotid artery ascended anterolaterally to the left in front of the trachea and divided into the external and internal carotid arteries (Fig. 1). The external diameter of the right common carotid artery at its origin, located approximately 5.10 mm distal to the origin of the left common carotid artery, was 11.35 mm (Table 1). After arising from the right side of the anterior wall of the aortic arch, it ascended almost vertically along the right side of the trachea (Fig. 1). The external diameter of the right subclavian artery at its origin, located 13.30 mm distal to the origin of the right common carotid artery, was approximately 14.40 mm (Table 1). The external diameter of the right vertebral artery, the first branch of the right subclavian artery at 32.60 mm from the origin, was 5.5 mm at its origin (Table 1, Fig. 2). The retroesophageal left subclavian artery, the fourth branch of the aortic arch, had an external diameter of 14.10 mm at its origin (Table 1). This artery originated approximately 26.70 mm distal to the origin of the right subclavian artery and 35.40 mm posterior to the origin of the left common carotid artery. It passed upward, posterolaterally to the left, behind the trachea and the esophagus (Fig. 1). The left vertebral artery, the first branch of the left subclavian artery at 44.40 mm from the origin, had an external diameter of 2.15 mm at its origin (Fig. 2) and passed into the transverse foramen of C6.
Discussion
Developmentally, the aortic arches result from the formation of paired ventral aortas, which arise from the summit of the truncus arteriosus and pass cephalad and ventral to the primitive pharynx [1, 2]. At the same time, dorsal aortas develop dorsolateral to the pharynx. Caudally, the dorsal aortas fuse to form a common vessel, which is the future descending aorta. These arteries are joined successively by 6 pairs of arches. The subclavian arteries originate from the seventh intersegmental arteries bilaterally and the vertebral arteries originate from the longitudinal anastomoses between these intersegmental arteries. The anomalies of branches arising from the aortic arch are caused by variations in the extent of fusion and absorption of some of the aortic arches into the aortic sac; the number and type of branches arising from the arch are determined by this process [3, 4]. These anomalous origins and the distribution of the large aortic arch vessels can cause changes in the cerebral hemodynamics that may result in cerebral abnormalities. Detection of these anomalous origins is significant for diagnostic purposes prior to surgery involving supra-aortic arteries.
A right-sided aortic arch has been reported in a case of tetralogy of Fallot [5] and the incidence of a right-sided aortic arch has been reported in 0.05-0.1% of radiological findings and 0.04-0.1% of autopsy specimens [5, 6]. Based on Edwards' description [7], right-sided aortic arch anomalies with mirror image arch branches are classified as Type I, with aberrant left subclavian artery and Kommerell's diverticulum as Type II, and with isolated left subclavian artery as Type III. The incidence of these 3 types have been reported as 59%, 39.5%, and 0.8%, respectively. The abnormality in this case is a kind of Type II without Kommerell's diverticulum. Kommerell's diverticulum is common in persons with this anomaly, and is believed to be a remnant of the distal part of the right dorsal aorta [8]. Concerning the developmental aspects, this anomaly is the result of regression of the left fourth embryonic arch proximal to the left common carotid artery, with persistence of the left dorsal aortic root and the left ductus arteriosus.
In this unusual case, the first branch to arise from the arch was the left common carotid artery, followed by the right common carotid artery and then the right subclavian artery. The left subclavian artery originated as the last branch and coursed upwards and posterior to the esophagus on the left side. The ductus arteriosus persisted on the left and connected the left subclavian artery to the left pulmonary artery, forming a vascular ring. Congenital anomalies of the aortic arch and its branches produce recognizable effects, largely through esophageal and tracheal distortion [9, 10]. However, cardiac anomalies produced no recognizable effects in this case.
In conclusion, the different branching pattern of the aortic arch observed in this study and the morphometric measurements obtained can assist surgeons in performing safe and effective vascular surgeries in the thoracic, head and neck regions.


 XML Download
XML Download