

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Increasing activity in the fields of cardiac and vascular surgery has served to revive interest in the developmental and adult anatomy of the aortic arch and its great vessels. The aortic arch is a continuation of the ascending aorta, being located in the superior mediastinum. Three branches, brachiocephalic trunk, left common carotid artery and left subclavian artery usually branch from the aortic arch. These branches may branch from the beginning of the arch or the upper part of the ascending aorta with varying distances between them. The brachiocephalic trunk later divides into right common carotid artery and right subclavian artery. Variations in the branching pattern of the aortic arch range from differences in the distance between origins of different branches to number of branches [1, 2].
The position of the aortic arch may vary across the population. Common origin of the carotid arteries (COCA) is a normal aortic arch variant found in approximately 11% of whites [3] with an even higher prevalence, up to 25%, reported in the African-American population [4]. In COCA, the brachiocephalic trunk and the left common carotid artery arise from a single trunk of the aorta. The present study reports the different types of branching patterns of the aortic arch.
Materials and Methods
The study was carried out in 75 cadavers of both sexes (40 male and 35 female), approximately aged between 45 to 70 years of Indian origin, at Government medical College Nagpur over a period of three years. The mediastinum was opened and the branching pattern of the arch of aorta was observed.
Results
In this study the most common aortic arch branching pattern type I was found in 58 (77.3%) of 75 specimens. In this pattern the three major branches; brachiocephalic trunk, left common carotid, and left subclavian originated independently from the arch of the aorta.
The aortic arch pattern type II was found in 11 specimens (14.66%) which had only 2 great branches. They originated from the upper convex surface of the aortic arch. The first was a common trunk designated the great trunk (GT), which incorporated the brachiocephalic trunk and left common carotid. The second was left subclavian, rising independently distal to the origin of the GT (Fig. 1). Accordingly the length of GT type II was further classified into two types. Type II A had long length near about 4-6 cm (as in Fig. 1) while type II B had very short GT so that left common carotid artery appears to start from the root of brachiocephalic trunk. Out of 11 specimens of type II, four were of type II A and seven were of type II B (Fig. 2).
In six cadavers (8%) an additional artery was noted in addition to the common three branches. The additional branch was traced and found to be the left vertebral artery. It had an independent origin from the aortic arch. It was located between the origins of the left common carotid and the left subclavian arteries. This type was noted as type III. These four branches had their origin from the upper convex surface of the arch. The sequence of the four arteries from the arch, from right to left was brachiocephalic trunk, left common carotid, left vertebral and left subclavian artery (Fig. 3).
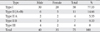
The details of types of aortic arch pattern with respect to sex and numbers of cases is given in Table 1. For radiological comparison of these types of aorta, angiography images (Fig. 4) of aorta were obtained from intervention radiology department of our college. No other noticeable variations on the branching pattern of the great blood vessels were found.
Discussion
Knowledge of variations in the branching pattern of the aortic arch is of great importance in patients who have to undergo four vessel angiography, aortic instrumentation, or supra aortic thoracic, head and neck surgery [5]. In addition, knowledge of abnormal branches originating from the aortic arch is also important in the diagnosis of intracranial aneurysms following subarachnoid haemorrhage [6]. A variant of origin and course of a great vessel arising from the aortic arch is of great clinical value, because lack of knowledge of these variations may lead to serious surgical complications during procedures occurring in the superior mediastinum and the root of neck. Variations in the branching pattern of the arch of aorta are likely to occur as a result of the altered development of certain aortic arch arteries during the embryonic period of gestation.
The six pairs of aortic arches are a series of vessels that connect on each side the aortic sac with the corresponding dorsal aorta. At a later developmental stage, the aortic arches are both reduced in number and extensively transformed, and finally an asymmetric blood supply system is achieved. The first and second aortic arches largely disappear by the time the third to sixth arches develop. The left limb of the aortic sac normally forms the part of the arch of aorta that intervenes between the origins of the brachiocephalic trunk and the left common carotid artery. If the aortic sac fails to bifurcate into right and left limbs, then the variations on the branching pattern of arch of aorta may occur, as observed in present study. The proximal part of the third aortic arch normally gets extended and absorbed into the left horn of aortic sac. If it gets absorbed into the right horn of the aortic sac, that also results in a variable branching pattern [7, 8]. Direct origin of the left vertebral artery from the upper convex surface of the arch of aorta between the origins of the left common carotid and left subclavian arteries may be explained as increased absorption of embryonic tissue of the left subclavian artery between the origin of the arch of aorta and the vertebral artery. Variations, when there are more than three branches originating from the arch of aorta may include the vertebral arteries [9, 10].
According to Adachi [11], in about 80.0% of individuals, three branches arise from the arch of aorta: the brachiocephalic trunk, left common carotid artery, and left subclavian artery. Adachi classified this branching pattern as type A. Another 11% have a common trunk incorporating the left common carotid artery and the brachiocephalic trunk leaving only two branches originating from the arch of aorta, Adachi's type B. The pattern, type C, has the left vertebral artery, a fourth branch of the arch of aorta, originating proximal to the left subclavian artery. Williams and Edmonds [4] reported finding variations in arch vessels after dissecting 407 human cadavers: 191 American whites and 216 blacks. According to their report, the frequencies of arch vessel variations in white and black populations were 17.8% and 37.8% for common brachiocephalic trunk, 2.6% and 2.0% for isolated left vertebral artery, and 1.0% and 0% for aberrant right subclavian artery, respectively. According to Anson and McVay [12], the normal three branched arrangement of the aortic arch was found in 64.9%. An arrangement distinguished by reduction in the number of stems to two, both common carotid arteries arising from the innominate occurred in 27.1%. The left vertebral artery was the additional vessel arising from the arch in 2.5%. In our study we found the following variations with different percentages: 77.3, 14.6, and 8%, respectively. The present study on Indian cadavers may provide adequate information on the branching pattern of arch of aorta to catheterize the same and its branches for safely performing endovascular surgery.
It has been reported that anomalies of the aortic arch branching pattern could lead to cerebral abnormalities by altering the pattern of flow in cerebral vessels [13]. All people included in the study lived apparently healthy lives up to 45 to 70 years. We studied the death history and death certificates of the cadavers used in this study and tried to find a relation of branching pattern of aorta with cerebro-vascular disease. Type I is normal branching pattern of the aorta in which out of 58 cadavers, 7 (12%) were diagnosed with cerebro-vascular disease, while in the case of variant branching pattern, type II and type III, 4 (23.5%) cadavers out of 17 had cerebro-vascular disease. In type II pattern, origin of left common carotid artery is slightly shifted to right side so that it is incorporated with brachiocephalic trunk and comes in a straight line with ascending aorta. This may be the reason to increase blood flow in left common carotid artery. In type III, direct origin of left vertebral artery from arch of aorta increases blood flow in left vertebral artery. This direct (straight line) flow of blood from aorta to brain or imbalance of flow of blood on left and right side at circle of Willis may be the cause of increased incidence of cerebro-vascular diseases in cadavers having type II and type III pattern of aortic arch.




 XML Download
XML Download