

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Neonatal chylous ascites is a very rare condition; the exact incidence of neonatal chylous ascites is unknown.1 Congenital chylous ascites can occurred from a variety of reasons. The most common cause (45–60% cases) is the malformation of the lymphatic vessels.2 Half of neonates, not mentioned above, the chylous ascites is thought to be due to delayed maturation of the lacteals, called “leaky lymphatics.”2 Another reason (20–25% cases) is obstruction of the lymphatics due to external compression, such as malrotation, intussusception, incarcerated hernia, enlarged lymph nodes and malignancy.2 In some cases (15–20% cases), it is caused by trauma during surgery, accidents or child abuse.2 We reported a rare case of ileal atresia presenting with massive chylous ascites and bilateral hydrocele at birth.
Case
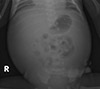
We report a male neonate with ascites and huge bilateral hydrocele who was born by caesarean section at 38 weeks of gestation with a weight of 3,360 g (50–75 percentile), height of 51.0 cm (75–90 percentile), and head circumference of 33.5 cm (50–75 percentile). The antenatal ultrasonography performed at 37+6 weeks of gestation showed ascites and huge bilateral hydrocele. The ascites depth of 2.3 cm was detected by antenatal ultrasonography and ascites was not turbid. (Fig. 1) The Pleural effusion, pericardial effusion, or edema of subcutaneous tissue was absent. The antenatal ultrasonography showed no evidence of hydrops fetalis. Fetal heart rate decreased, the baby was born by emergency caesarean section. At birth, the patient manifested hypotonia, massively distended abdomen and bilateral hydrocele (Fig. 2). In addition, he had no spontaneous breathing and no crying. The patient was warmed and secretions were cleared. After positive pressure ventilation, the pulse rate was under 100 beats per minute, without respiratory effort and cyanosis persisted. The 1-minute Apgar score was 2, and 5-minute Apgar score was 3. Endotracheal intubation was performed, and the baby was transferred to the neonatal intensive care units (NICU). On the physical examination, there was no meconium staining on the newborn's skin, no hepatosplenomegaly, nor palpable mass. The neonate had a white blood cell count of 12.66×109/L with 62% neutrophils, and 29% lymphocytes, and platelet count of 139×109/L. In a blood sample, sodium was 137 mEq/L, potassium 4.8 mEq/L, chloride 101 mEq/L, aspartate transaminase 106 IU/L, alanine aminotransferase 16 IU/L, cholesterol 27 mg/dL, triglyceride 15 mg/dL, total protein 4.8 g/dL, and albumin was 2.5 g/dL. C-reactive protein was 0.32 mg/dL in a first laboratory test on the first day of life. From the venous blood gas analysis (VBGA), venous blood pH was checked as 7.160, PCO2 was 41.0 mmHg, base excess was -14 mmol/L. Seven hours after birth, abdominal distension worsened. On the abdomen x-ray, the bowel gas was located centrally (Fig. 3). Abdominal ultrasonography revealed meconium peritonitis with a large amount of complicated ascites suggestive of probable bowel perforation. Thickening of the small bowel loop was seen especially from the bowel loops in the right lower quadrant area (Fig. 4). The possibility of underlying bowel pathology like atresia or internal hernia was mentioned from that abdominal ultrasonography. There was no evidence of mid-gut volvulus such as the ‘whirlpool’ or ‘coffee bean’ sign. Large amount of complicated ascites was seen in both scrotal sac areas. Both kidneys appeared normal in size with normal echotexture. Otherwise, no definite abnormality was detected in both kidneys. The urinary bladder showed normal contour and wall thickness.
Exploratory laparotomy was performed on the day of birth. A large amount of chyle (approximately 200 mL) was found in the peritoneal cavity between the bowel loops. An additional 120 mL of chyle was removed from both scrotal sacs. The color of chyle was ivory yellow with whitish debris. The analysis of fluid from peritoneal cavity and both scrotal sacs was not conducted. The flow of chyle from the peritoneal cavity through the inguinal canal had resulted in huge bilateral hydrocele.
Ileal atresia had occurred 7 cm above the ileocecal valve. The proximal small bowel was disconnected, and the distal small bowel loop ended in a blind loop (Fig. 5). There was no evidence of malrotations or dilatation of lymphatics. Laparotomy with subsequent histopathology confirmed the diagnosis. Anatomical origin was the small intestine, which showed necrotic tissue and scanty amount of viable small intestine wall (Fig. 6). The pathologic findings from the segmental resection of small intestine indicated submucosal and subserosal congestion with chronic inflammation, fibrinous exudate and micro calcifications at serosal surface with meconium peritonitis. Segmental small bowel resection and double barrel ileostomy was performed, and the patient was transferred to the NICU.
Bowel motility was observed on postoperative day 7 (postnatal day 8), and feeding was initiated. He was weaned off oxygen on postnatal day 15. Gastrograffin enema for evaluation of the proximal and the distal bowel loops was done on postnatal day 22. The diameter of rectum was intact; whereas, the diameter of colon loop above rectum was decreased, consistent with an underused micro colon.
The level of conjugated bilirubin increased to 4.2 mg/dL on postnatal day 6. The hepatobiliary scan showed delayed hepatic excretion. Ursodeoxycholic acid and phenobarbital were administered.
Brain magnetic resonance imaging was taken on postnatal day 19. On the diffusion weighted image, there are lesions with high signal intensity and diffusion restriction at splenium and posterior body of corpus callosum. It could be possible from the hypoxic ischemic injury. There are T1 high, T2 low punctate lesions at white matter of the both frontoparietal lobes. It could be thought petechial hemorrhage.
The patient was discharged from the hospital on postnatal day 46 with a weight of 3,450 grams (<3 percentile), height of 53.0 cm (3–5 percentile), and head circumference of 35.0 cm (<3 percentile). The level of direct bilirubin normalized at 3 months after birth. The patient was readmitted for repair of ileostomy on postnatal day 86 with a weight of 5,100 grams (3 percentile), height of 58.5 cm (10–25 percentile). Closure of stoma of small intestine was done and he has been doing well at outpatient follow-up.
Discussion
Fetal ascites is defined as the accumulation of fluid in the peritoneal cavity. It is caused by immune hydrops fetalis, non-immune hydrops fetalis, cardiac malformations, congenital infections, gastrointestinal anomalies and genitourinary anomalies.3 Ascites can be accompanied by other abnormalities, such as structural malformations or genetic syndromes.4 On ultrasonography examination, fluid accumulation appears as echo-free fluid outlining the falciform ligament, umbilical vein, between the bony rib cage and viscera, and in the peritoneal cavity between the bowel loops.4
Neonatal chylous ascites is a very rare condition.1 Congenital chylous ascites can occurred from a variety of reasons. The 1st most common cause is the malformation of the lymphatic vessels.2 The 2nd most common cause is delayed maturation of the lacteals, called “leaky lymphatics.”2 Another reason is obstruction of the lymphatics due to external compression, such as malrotation, intussusception, incarcerated hernia, enlarged lymph nodes and malignancy.2 In some cases, it is caused by trauma during surgery, accidents or child abuse.2
Paracentesis is both a diagnostic and therapeutic step, and lymphoscintigraphy is used to reveal the lymphatic anatomy.1 Enteral feeding with a medium chain triglyceride formula can be started, but nil per os (NPO) and total parenteral nutrition may be necessary to reduce chylous flow in severe or complicated cases.1 The goal of the surgical management is to find and fix the lymphatic leak.1 Patients with chylous ascites have a risk for recurrence, but there were no recurrences in our case.
The proximal small bowel was disconnected, and the distal small bowel loop ended in a blind loop (Fig. 5). Lymphatic drainage from that cross section of the proximal small bowel might be a cause of chylous ascites. The color of chyle was ivory yellow with whitish debris. There was no meconium stained ascites or soiling of the peritoneal cavity, it was thought that the disconnection of proximal small bowel was happened just before the surgery.
In the republic of Korea, there was one similar case report of a neonate with massive chylous ascites and hydrocele.5 In the report, a male neonate was born at 36 weeks of gestation with a weight of 2,990 grams.5 Ascites was detected on antenatal ultrasonography at 35 weeks.5 On the day of birth, paracentesis was done and the ascites was chyle.5 Gastrograffin enema was done on postnatal day 4.5 From that study congenital ileal atresia was seen, and then segmental small bowel resection and ileocolostomy was done.5
From the case we mentioned above, paracentesis was done on the day of birth.5 In my case, paracentesis was not conducted, but exploratory laparotomy was performed on the day of birth. From the gastrograffin study, congenital ileal atresia was seen in the case we mentioned above, but in my case gastrograffin study was done after exploratory laparotomy. We had few information from the study except underused micro colon.
Congenital small bowel atresia of the duodenum, jejunum or ileum is the most common cause of neonatal bowel obstruction, with incidence ranging from 1.3 to 2.8 of 10,000 births.6 Congenital small bowel atresia occurs mostly in the duodenum and less frequently in the jejunum or ileum.7 The signs of jejuno-ileal atresia include abdominal distension, bilious vomiting, jaundice, and no passing of meconium on the first day of life.7 The differential diagnosis of gastrointestinal obstruction in neonates includes esophageal atresia, pyloric stenosis, malrotation with midgut volvulus, intestinal stenosis, intestinal atresia, duodenal duplication, annular pancreas, foreign body obstruction, and Hirschsprung disease.7
If bowel dilatation and ascites are detected, small intestinal obstruction must be considered in the diagnosis. Prenatal diagnosis of gastrointestinal anomalies is very important to perinatal management, allowing delivery in centers in which radiologic imaging and surgical intervention are available. Collaborative effort of obstetricians, radiologists, neonatologists and pediatric surgeons could lead to early intervention, which can reduce morbidity and improve outcomes.





 XML Download
XML Download