

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gelatinous transformation of bone marrow, which is also known as marrow starvation and serous atrophy of the bone marrow, is a rare and poorly understood condition. Its histological features include hypoplasia of fat cells with focal loss of hematopoietic cells and accumulation of extracellular gelatinous substances, such as mucopolysaccharides (1). A heterogeneous group of devastating underlying diseases are known to cause this condition (12). Here, we present a female patient with gelatinous transformation of the bone marrow, who was initially diagnosed with diffuse bone metastasis or hematologic malignancy on magnetic resonance (MR) imaging, without confirmation of the underlying disease.
CASE REPORT
A 75-year-old female patient presented to the orthopedic clinic with complaints of low back pain and a weight loss of 5 kg over a 3-year period. She presented with thoracolumbar kyphosis and complained of bilateral claudication of the thigh and calf after walking for 5 min. She was 148 cm tall and weighed 31 kg (body mass index: 14.2 kg/m2).
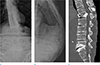
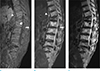
Radiographs of the lumbar spine revealed kyphosis and scoliosis of the thoracolumbar spine with an anterior wedged compression of the L1 vertebral body (Fig. 1a, b). Computed tomography (CT) revealed a burst fracture of the L1 vertebral body, with retropulsion of bone fragment, and bulging discs at all levels of the lumbar spines with decreased disc height (Fig. 1c). An MR image of the lumbar spine (1.5T MR scanner, MAGNETOM Avanto, Siemens Healthcare, Erlangen, Germany) revealed diffuse hypointense signals on T1-weighted images (T1WI) and irregular patchy geographic hyperintense signals on T2-weighted images (T2WI) at the bone marrow, relative to skeletal muscle, involving the entire vertebral column included in the MR image (Fig. 2). Additionally, sagittal fat-saturated T2WI of the lumbar spine showed hyperintense bone marrow signals. A diffuse lack of fat tissue was observed on T1WI in and around the muscles and the visceral and subcutaneous fat showed hyperintense signal on T2 and fat-saturated T2 sequences.
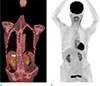
MR imaging suggested neoplastic conditions, including metastasis and hematologic malignancy, as the most likely differential diagnoses. Diffuse hyperplasia of hematopoietically active marrow, involving the entire vertebral column, was another possibility. Hence, whole-body 18F-fluorodeoxyglucose (FDG)-positron emission tomography (PET)-CT was performed for a diagnostic work-up of a putative underlying hidden malignancy. However, no hypermetabolic focus was seen to suggest primary malignancy or distant metastasis (Fig. 3).
Although no imaging evidence of malignancy was found, confirmation of the bone marrow pathology was essential, as a primary malignancy with low FDG uptake could not be excluded. Bone marrow biopsy was performed at the posterior superior iliac crest, bilaterally. Pathological examination indicated gelatinous transformation of the bone marrow, rather than a malignant marrow-replacing lesion (Fig. 4). The extracellular gelatinous substance tested positive for Alcian blue stain.
These results prompted us to refocus on the patient's clinical history for underlying disease. Blood examination revealed moderate neutropenia (absolute neutrophil count, 950/µL; reference range: 1500–7700/µL) and anemia (hematocrit, 31%, with a reference range of 37–47%; hemoglobin, 10.8 g/dL; reference range: 12–16 g/dL). Serum albumin was normal (3.9 g/dL; reference range: 3.4–5.3 g/dL). The total protein level was slightly below the lower limit of the normal range (6.0 g/dL; reference range: 6.9–8.3 g/dL). The body mass index was 14.2 kg/m2; however, investigations revealed no clinical history of devastating disease associated with nutritional deficiency. The patient had no previous or current clinical history of alcoholism, anorexia nervosa, vegetarianism, or chronic infection. Gastrointestinal and pancreatobiliary problems were absent during regular follow-up, 3 months earlier, which involved endoscopy and laboratory tests, and during the initial routine clinical work-up at our institution. She had no heart problem, hematologic malignancy, metastasis, or metabolic disorder, such as diabetes mellitus (fasting serum glucose level, 83 mg/dL; reference range: 70–110 mg/dL).
DISCUSSION
We misinterpreted the patient's spinal MR images as indicative of a malignant marrow-replacing lesion. Spinal MR images of patients with gelatinous transformation of the bone marrow show features similar to those of a bone-marrow replacing lesion involving the entire vertebral column. Thus, in the absence of underlying diagnosis and the presentation of rare and unfamiliar clinical pathology, the imaging results can lead to a misdiagnosis.
Gelatinous transformation of bone marrow is not a disease per se, but indicates an underlying illness that starves the bone marrow, particularly the fatty marrow (12). The pathogenesis involves accumulation of acid mucopolysaccharides, i.e., hyaluronic acids replacing fat cells of the bone marrow in an energy-deficient state (3). The incidence of this condition is approximately 0.2% (1). The diseases associated with gelatinous bone marrow transformation include infections (48.1%), such as AIDS/HIV; nutritional deficiencies (7.6%) such as alcoholism, anorexia nervosa, and vegetarianism; and hematological conditions (26.2%) (12), which were absent in our patient. Although our patient was slightly anemic, the degree of anemia did not correlate with the extent of bone marrow transformation, and the role of anemia in this condition is unclear. Furthermore, because the acid mucopolysaccharide deposits in the bone marrow may interfere with hematopoietic proliferation, anemia may result from, rather than cause gelatinous transformation (123). Although the cause of this patient's malnourishment remains unclear, this case does highlight that bone marrow transformation can occur in patients with unexplained malnutrition, in the absence of an underlying cause.
MR findings showed a marked increase in signal intensity on T2WI scans, indicating a prominent increase in free-water content. These abnormal water-like signal intensity patterns in the bone marrow are attributed to the accumulation of acid mucopolysaccharides in hypocellular bone marrow spaces with fatty atrophy (4). These patterns are predominantly distributed at the peripheral skeleton, in a diffuse manner, whereas in the vertebral marrow, heterogeneous patterns are seen on T2WI scans, compared with uniformly hyperintense signals of the axial skeleton in diffuse neoplastic infiltration. MR imaging signals of this patient were diffusely hypointense on T1WI scans, mimicking a devastating neoplastic condition associated with malignant cell infiltration (5). However, irregular and patchy hyperintense signal intensity on T2WI scans with poor fat saturation on sagittal fat-saturated T2WI scans, and a concurrent disappearance of whole body subcutaneous and visceral fat including lack of intra- and intermuscular fat tissue along with severe underweight, suggests gelatinous bone marrow transformation rather than a neoplastic condition. A diffuse fat-depleted state of this patient distinguishes the patient's condition from malignant changes.
Gelatinous transformation of the bone marrow has also been seen in malignant conditions, because of the seromucinous and gelatinous hyaluronic acid-rich substances, which replace the bone stroma (267). Therefore, the possibility of malignancy, such as hematologic neoplasm or diffuse bony metastasis of unknown primary origin, could not be excluded. Hence, it is crucial to exclude hidden malignancy, using diagnostic imaging tools, such as PET-CT, before a diagnosis of gelatinous bone marrow transformation is made in a patient without a known underlying disease. PET-CT revealed no focal lesion of FDG uptake on scanned images, including the entire vertebral column, which excluded the possibility of malignant conditions in our case. To our knowledge, only one case of gelatinous bone marrow transformation has been reported previously based on PET-CT findings, which showed a poor sensitivity for the detection of gelatinous components (8). Moreover, an investigation of gelatinous transformation of bone marrow has yet to be reported based on simple radiography, CT, MR, and PET-CT images (4910).
In conclusion, the present case suggests that gelatinous bone marrow transformation should be considered in the differential diagnosis when MR imaging reveals diffuse bone marrow-replacing lesions and malnutrition is suspected, in the absence of an a detectable underlying disease such as cancer.

 XML Download
XML Download