

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
soft tissue sarcoma is a rare tumor that has a prevalence of approximately 30 people per each million (1). Among them, myxoid liposarcoma arising from the mesentery is even more rare and has been reported in only 17 cases thus far in the medical literature (2). Liposarcomas show various radiologic and histopathologic features depending on their internal components. Herein we report ultrasound, computed tomography (CT), and magnetic resonance (MR) image findings for a case of myxoid liposarcoma originating from the mesentery that mimics fibromyxoid sarcoma, and discuss the imaging features that can differentiate this tumor from other mesenteric tumors which contain a myxoid component.
CASE REPORT
A 49-year-old male patient was admitted to our hospital with an incidental peritoneal mass abutted to the jejunum on a regular follow-up abdominal CT. The review of his past history indicated that he underwent a surgical resection for a mesenteric tumor 2 years ago. At that time, the pathologic diagnosis of the resected mesenteric tumor was a low-grade fibromyxoid sarcoma. There was no palpable mass evidenced in the physical examination, and no new complaints such as weight loss, abdominal pain, diarrhea, constipation and vomiting were submitted by the patient. The laboratory findings were within normal range.
The latest contrast-enhanced abdominal CT images showed a 5-cm-sized well-defined solid mass abutting the antimesenteric border of the jejunum. The tumor had low attenuation on the pre-contrast CT images and a heterogeneous enhancement pattern on the arterial phase and persistent enhancement on the portal venous phase (Fig. 1).
To evaluate this incidentally detected mass, MR imaging was performed. The tumor revealed a well-defined low signal intensity mass which contained small tiny high signal intensity foci on the chemical shift in-phase and signal drops on the out-of-phase T1-weighted MR images (Fig. 2a, b), and heterogeneous bright high signal intensity components mimicking a cystic tumor on the T2-weighted MR images (Fig. 2c). There was no definitive fat suppressed lesion on the fat saturated T2-weighted MR images (Fig. 2d). The tumor showed high signal intensity on the diffusion weighted images with a high b-value (800 s/mm2) (Fig. 2e) and low value on the apparent diffusion coefficient (ADC) map (Fig. 2f), which suggested diffusion restriction.
Those lesions mimicked cystic masses on the MR images, but showed solid components on the CT and ultrasound images. Those findings suggested a myxoid component of the tumor. As such, we suspected myxoid tumors such as fibromyxoid sarcoma, myxoid liposarcoma, myxoid leiomyosarcoma and myxoma. Initially, our first impression was the recurrence of a low grade fibromyxoid sarcoma of the mesentery based on his previous surgical history. Also, the tumor was located in the mesentery as before and had similar radiologic findings compared with that of 2 years ago (Fig. 3).
But, there were some distinct radiologic findings on the MR images. The tumor showed multiple small tiny hyperintense foci on the in-phase T1-weighted images and signal drops on the out-of phase T1-weighted MR images. Those findings suggested tiny intratumoral fat components even though there was no fat suppressed portion in the tumor on the fat saturated T2-weighted MR images. Signal drops foci can indicate the diagnosis of fat containing solid tumors. Taken together, our impression was changed to myxoid liposarcoma.
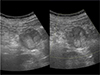
The patient underwent an ultrasound examination for a needle biopsy. The lesion showed a well-margined heterogeneous hypo- and hyperechoic mass attached to the jejunum. No internal vascularity was visible on the color-Doppler ultrasound (Fig. 4).
An operation for the mesenteric tumor was performed. In the histopathologic exam, the surgical biopsy result of a mesenteric mass was different from the previous biopsy results obtained 2 years ago. The specimen exhibited multiple fatty vacuoles and lipoblasts with a myxoid spindle cell mesenchymal background and a prominent vessel structures (Fig. 5). The mesenteric mass was a myxoid liposarcoma. More interestingly, a retrospective histopathologic examination of the specimens 2 years ago revealed that the previous tumor was proven to be a myxoid liposarcoma. The former specimen had fewer lipoblasts and fatty vacuoles, so it mimicked fibromyxoid sarcoma. The patient experienced no complications during his postoperative course and no recurrence was detected during follow-up visits.
DISCUSSION
Liposarcoma is a group of tumors arising from the mesenchymal cells. According to the 2013 World Health Organization classification of tumors of soft tissue and bone, it can be divided into 4 subtypes: well-differentiated (or atypical lipomatous tumor), dedifferentiated, myxoid, and pleomorphic liposarcoma (1). Myxoid liposarcoma accounts for about 30% to 35% of all liposarcomas and is the second most common subtype of liposarcoma.
The radiologic findings of mesenteric origin myxoid liposarcoma are varied. According to Dufay et al. (3), myxoid liposarcoma of the mesentery on CT and MR images shows heterogeneous attenuation and a signal intensity with fat components intermixed with the zones of the denser tissue. The borders are poorly defined and often infiltrating. The contrast enhancement pattern is heterogeneous and has a persistent to delayed phase (4). Shin et al. (5) have demonstrated that myxoid liposarcoma of the mesentery shows amorphous or linear high signal intensity on the T1-weighted images and isointensity on the T2-weighted images, which is consistent with fat composition. In addition, the chemical shift MR sequence has been reported to be useful in the diagnosis of myxoid liposarcoma. These MR imaging findings were also found in our case. Multiple small foci that showed high signal intensities were detected on the in-phase chemical shift T1-weighted image whereas corresponding small hypointense foci were detected on the out-of-phase T1-weighted MR image. These signal drops suggested the presence of small fat containing foci in the tumor. Also, use of fat-suppression or fat-saturation techniques can be helpful to detect the adipose content in myxoid liposarcoma (6). Some myxoid liposarcoma may not exhibit the typical findings but show a cyst-like appearance on MR imaging. The reason for the mimicking cysts is that myxoid components show an MR signal intensity similar to that of fluid. An ultrasound is useful to differentiate the solid mass from cystic lesions (4).
On the CT scan, myxoid liposarcoma is similar to low-grade fibromyxoid sarcoma because the mucinous component may be seen as having a low density compared to the muscle and shows heterogeneous attenuation and an enhancement pattern (7). However, MR imaging can differentiate the liposarcoma when a fat component is observed in the tumor. Otherwise, it is difficult to distinguish between those two tumors.
In our case, a histopathologic examination at the time of the first operation revealed few fatty vacuoles in the mass, which was misdiagnosed as low grade fibromyxoid sarcoma. However, the recurrent mass had multiple small lipid vacuoles and was finally diagnosed as myxoid liposarcoma. Histologically, myxoid liposarcoma has immature lipoblasts with a small amount of adipose tissues and rich mucinous matrix. In fact, up to 50% of the cases of myxoid liposarcoma involved tumors that have varying degrees of mucinous cells which makes it difficult to differentiate them from low-grade fibromyxoid sarcoma (45).
Myxoid leiomyosarcoma and myxoma should be included in the differential diagnosis of our case because it can appear as a cystic mass on the T1- and T2-weighted MR images (8). Those two tumors usually show various imaging patterns so the differentiation of myxoma or myxoid leiomyosarcoma from myxoid liposarcoma is quite difficult. The fatty components in myxoid liposarcoma could also facilitate differential diagnosis (4).
Other mesenteric tumors that have to be included in the differential diagnosis are lymphoma and desmoid tumor. Lymphomas usually show a homogeneous CT attenuation with variable enhancement patterns. A helpful consideration when diagnosing lymphoma is the presence of enlarged lymph nodes around the tumor or other sites. A desmoid tumor appears to have low attenuation on CT due to the mucin component and shows a peripheral enhancement with some linear enhancement patterns at the central portion of the tumor (9).
Primary mesenteric myxoid liposarcoma has many aggressive features and only extensive surgical resection can treat this malignant tumor. However, there are many case reports about the recurrence of mesenteric myxoid liposarcoma despite complete surgical resection (10).
In conclusion, if there is a heterogeneously enhancing solid tumor with a myxoid component at the mesentery and signal drop foci are present on the chemical shift MR images, myxoid liposarcoma should be included in the differential diagnosis.




 XML Download
XML Download