

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Herniated intervertebral disc (HIVD) and neurogenic tumor are very distinctive disease entities with different origins, pathologies, and treatments. However, around the intervertebral foramen, the relatively confined space and the spatial proximity between the intervertebral disc and the spinal nerve root often makes it difficult to distinguish HIVD from neurogenic tumors (12). Here, we present a case of extraforaminal intervertebral disc extrusion (IDE), which mimicked a peripheral nerve sheath tumor. We then review relevant radiologic aspects to differentiate the two disease entities.
CASE REPORT
A 55-year-old male visited an outpatient clinic for low back pain and radiating pain to the left posterior thigh. He had chronic low back pain and occasional radiating pain, which became aggravated after he jumped down from a height of 2-meters, about one month prior to his examination. He formerly had claudicant symptoms; however, due to the jump, the symptoms aggravated. Additionally, he complained constant numbness and tingling at the right anteromedial thigh.
In the physical examination, straight-leg raises caused radiating pain to the left posterior thigh. When compressing the spinous processes to induce shear force between the adjacent vertebrae, all vertebrae at levels L3 and below provoked pain. Paraspinal muscle tightness and tenderness was present along the whole lumbar spine, bilaterally. Gluteal muscle tenderness was more prominent on the left side, and the manual muscle test showed no focal motor deficit.
The radiograph of the lumbosacral spine showed compression fracture at L1 and L3 vertebrae, disc space narrowing at L2/3 and L5/S1 levels, and grade 1 retrolisthesis of L3/4. The magnetic resonance (MR) image revealed diffuse spondylotic features that could be inferred by the radiograph. A noteworthy finding that correlated with the patient's chief complaint was an asymmetric bulging disc at the L5/S1 level with compression of the left S1 nerve root. Interestingly, we found a mass at the right extraforaminal zone of L3/4 level, sized about 2 centimeters (Fig. 1). This mass was concordant with the dysesthesia of the right thigh.
We performed a transforaminal epidural steroid injection at the left S1 root. Afterwards, radiating pain to the left posterior thigh considerably improved. We considered the extraforaminal mass at the L3/4 level a neurogenic tumor, possibly schwannoma. As such, we conducted surgical excision.
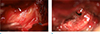
Under general anesthesia with neuromonitoring, we performed the paramedian approach to excise the mass. During the mass dissection, we realized the mass had no connection to the nerve root and had continuity with the L3/4 intervertebral disc (Fig. 2). Accordingly, we performed an L3/4 discectomy.
The pathologic finding of the mass was fibrovascular collagenous tissue with degenerated cartilage and peripheral neural component. This finding was more suggestive of degenerated annulus and nucleus pulposus, rather than a peripheral nerve sheath tumor. The dysesthesia of the right thigh improved after the surgery.
DISCUSSION
On account of its high soft-tissue resolution, MR imaging would be the best choice for differentiating HIVD from neurogenic tumor. In the MR image, the signal intensity and morphology of the herniated disc material can vary according to the chronicity of the lesion, inflammatory response or granulation surrounding the extruded material, adjacent anatomic structures, and so on. Thus, signal intensity and the morphology of a lesion cannot ensure the diagnosis, and the continuity or the adjacency with the intervertebral disc space. Disc space is one of the most important features of HIVDs (3). In cases of extruded or sequestered discs, which have considerable displacement from its origin, they can be confused with other pathologies.
Nerve sheath tumors usually have hypo- or isointensity in T1 weighted images, and high signal intensity in T2 weighted images (4). The morphology conforms to solid adjacent structures; however, when the surrounding environment is relatively redundant, nerve sheath tumors would be round in the transverse plane, as a result of concentric expansion (5). Special signs, such as a split fat sign, target sign, or fascicular sign can be observed. However, none of these signs are a pathognomic feature (6). A nerve entering and exiting the mass is virtually pathognomic, but this finding is often impossible to observe in small nerves (7). In 70% of schwannomas and in 30% of neurofibromas, the capsule, a thin rim of low-signal intensity in T2 weighted image, can be observed. The capsule represents the epineurium or remaining nerve encapsulating the mass (8).
There were several features of the MR image of the patient that misled us to the diagnosis of neurogenic tumor. The current case showed isointense T1 and high T2 signal intensity, which is common in peripheral nerve sheath tumors. Extruded discs contain degenerated disc materials and annular fibers, which are of low-signal intensity in T2 weighted images (9). Thus, most extruded disc have some portion of low-signal intensity. The location of the lesion did not favor HIVD. The most frequent locations where disc herniations occur are the inside of the spinal canal, followed by the intervertebral foramen. Extraforminal disc herniations are relatively uncommon (10).
The morphology of the lesion is unusual for an IDE. In the current case, the lesion showed a rather circular shape in all axial and sagittal images. An IDE is usually irregular in shape. Additionally, the T2-weighted image revealed a split fat sign, which is a hyperintense rim surrounding the lesion. This results from displaced fat tissue and a low-signal intensity contour, which resembles a capsule.
A contrast-enhanced MR image can be helpful in differentiating between extruded or sequestrated disc and peripheral nerve sheath tumors. The extruded or sequestrated disc represents a peripheral enhancement pattern, due to inflammatory changes and neovascularization surrounding the central non-enhancing cartilagenous portion (1). On the other hand, schwannomas usually show a homogeneous enhancement pattern and neurofibromas show a central enhancement pattern (6). Unfortunately, we did not perform a contrast-enhanced MR sequence in this case. Because we initially suspected the patient had HIVD, the MR image protocol without the contrast-enhancement sequence was performed. If we had performed a contrast-enhanced MR image, it may have aided us in differentiating an extruded disc from nerve sheath tumor.
Differentiating HIVD from neurogenic tumor is critical since the treatments for these conditions are distinct from each other. An HIVD should initially be dealt with using conservative methods. When medication and physical therapy fail, injections, such as transforaminal epidural steroid injections, can be tried. Here, based on our incorrect diagnosis, we conducted an open surgery to expose and excise the tumor. Considering the size of the extrusion and the nerve impingement by the lesion, surgery might have eventually been necessary. However, knowing it had been an IDE, we could have first considered less invasive methods, such as mini-open surgery or endoscopic excision. Since the treatment of neurogenic tumor is not an emergency, conservative treatments such as epidural steroid injections should have been tried prior to surgical excision. Were they successful, surgery might have been unnecessary.
In retrospect, there are several findings in the patient's MR image that imply IDE. Firstly, in reviewing the axial/sagittal images of the mass at the level of its largest diameter, the axial T2-weighted image reveals a fibrillary pattern originating from the intervertebral disc to the lesion. The alternating hypo- and hyper-intense lines correspond to the pathway through which the nucleus pulposus penetrate the frayed degenerated annulus (Fig. 1a, f). The sagittal image presents a more definite finding that indicates intervertebral disc lesion. The image shows an indentation in the mass lesion is at the level of the ring apophysis of the lower vertebra (Fig. 1c-e). This indentation is caused by the marginal ridge of the lower vertebra. From the image, we could have inferred that the annulus, which would normally separate the intervertebral disc space and the mass lesion, is disrupted. Were the annulus intact, the indentation of would correspond to the level of the bulged intervertebral disc not the vertebral ring apophysis. Moreover, in the sagittal T2-weighted image of the lateral aspect of the vertebra, the hypointense area at the level of the intervertebral disc shows invagination by isointense material, which implies annular disruption (Fig. 1f).
A few clinical points could have been made to make a correct diagnosis prior to the surgery. Detailed ex post facto history of the anterior thigh symptom was taken. The dysesthesia was intermittent, which became constant after the fall. A sudden aggravation of the symptom will be rare in cases of neurogenic tumor. Positive shear intolerance at L3 and below levels indicate mechanical back pain. However, this physical examination is non-specific and patients with focal lumbar pathology can have diffusely abnormal shear intolerance. The patient's chief complaint was low back pain and radiating pain to the left posterior lower extremity, and we considered this sign as a manifestation of the bulged disc at L5/S1 level.
In conclusion, we report a case of extraforaminal IDE resembling neurogenic tumor in the MR image. Prior to diagnosing neurogenic tumor around the intervertebral foramen, in the aspect of interpreting MR image, a thorough inspection of the relationship between the mass and the intervertebral disc space to rule out HIVD is necessary. Subtle findings, like a fibrillary pattern directed from the intervertebral disc to the lesion, disrupted annulus fibrosus, or indentation caused by the ring apophysis, are indicative of HIVD.

 XML Download
XML Download