

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
As breast magnetic resonance imaging (MRI) is being used more frequently to screening and diagnosis of breast malignancies, we often encounter various breast skin lesions appearing as skin thickening or enhancement. Although numerous studies have reported about the breast parenchymal lesions, the dermal lesions of the breast have largely been overlooked. The breast skin lesions may be incidental findings to be ignored, but sometimes the lesions are associated with breast cancer or other malignancies. Occasionally, the skin thickening or enhancement of the breast on MRI is the only finding to raise concern for tumor recurrence at the mastectomy site, treated or reconstructed breast of the breast cancer patient. In this article, we discuss the normal findings of the breast skin on MRI and demonstrate a spectrum of dermal lesions of the breast range from benign to malignant entities.
MRI Technique for Evaluation of Skin Lesions
The MRI scans were acquired with the patient in the prone position in a 1.5T scanner (Achieva; Philips Medical Systems, Best, The Netherlands) and a 3.0T scanner (Magnetom Verio; Siemens Medical Solutions, Erlangen, Germany) equipped with a breast coil. The MR images with the Achieva scanner were performed using the following sequences: sagittal, fat-suppressed, and fast spin-echo T2-weighted imaging sequence (TR/TE 6000/100 ms, flip angle of 90°, 30 slices, field of view [FOV] of 320 mm, matrix 424 × 296, number of excitations [NEX] of 1, 4 mm slice thickness with 0.1 mm interslice gaps, and acquisition time of 2 min 56 sec) and precontrast and postcontrast dynamic axial T1-weighted three-dimensional, fat-suppressed, fat-spoiled gradient-echo sequence (TR/TE 6.9/3.4, flip angle of 12°, 2.0 mm slice thickness with no gap, acquisition time of 1 min 31 sec) obtained before and at 0, 91, 182, 273, 364, and 455 sec after a rapid bolus injection of gadolinium-diethylenetriamine pentaacetic acid (Gd-DTPA) (Magnevist; Schering, Berlin, Germany) at 0.1 mmol/kg of body weight. The MR images with the Verio scanner were acquired using the following sequences: axial, turbo spin-echo T2-weighted imaging sequence (TR/TE 4530/93 ms, flip angle 80°, 34 slices with FOV 320 mm, matrix 576 × 403, 1 NEX, 4 mm slice thickness, acquisition time 2 min 28 sec) and pre- and postcontrast axial T1-weighted flash three-dimensional, VIBE sequence (TR/TE 4.4/1.7, flip angle 10°, 1.2 mm slice thickness with no gap, acquisition time 60 sec) obtained before and at 7, 67, 127, 187, 247, and 367 sec after a bolus injection of 0.1 mmol/kg Gd-DPTA.
In the conventional breast MRI including T2-weighted imaging sequence, precontrast and postcontrast dynamic axial T1-weighted sequences; we have to focus on the early enhanced T1 weighted image for detecting skin lesion and skin enhancement. In the supine MRI (chest of abdomen) as well as prone, skin lesion and skin enhancement could be detected.
Normal MRI Appearance of the Breast Skin
The skin is composed of three layers: the epidermis, dermis, and hypodermis, or the subcutaneous fat layer (Fig. 1a). The epidermis is indistinguishable as a separate layer from the dermis at imaging. The epidermis and dermis appear as a symmetric and smooth, with a thickness of 0.5-2 mm at MRI, except caudally where it may be slightly thicker due to its usual dependency. Although some investigators have noted that the normal skin may not enhance at MRI, the others have found that it is usually demonstrates mild thin enhancement (12) (Fig. 1b).
Malignancies Involving Skin
Inflammatory Breast Cancer
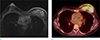
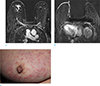
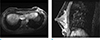
Inflammatory breast cancer (IBC) is a rare, highly aggressive form of primary breast cancer that comprises 1-6% of all the cases of breast cancer. Clinically, IBC is characterized by the rapid onset of swelling and enlargement of the breast. The overlying skin remains intact, but there is erythema that is often combined with a "peau d'orange" texture, local tenderness, induration and warmth. IBC is classified as T4d lesion; it is associated with a poor prognosis because of approximately 20% of cases of IBC already having metastasis at the time of presentation. Pathologically, any subtype of primary breast cancer may be present, but the dermal lymphatic vessels must be involved (345). MRI is the imaging tool of choice in evaluating patients with potential IBC. The MRI features of IBC are skin thickening and a reticular/dendritic pattern of parenchymal enhancement (Fig. 2). MRI showed significantly higher accuracy for depiction and delineation of a primary breast parenchymal abnormalities and skin thickening in IBC patients compared with conventional mammography and ultrasonography. Moreover, MRI is essential in treatment planning, as it supplies information of disease extent. Skin changes, global skin thickening or nodular or irregular skin foci, may occur in a different quadrant than that in which the underlying parenchymal mass is located (567). The majority of the kinetic pattern of the pathologic proven malignant skin lesions showed delayed persistent enhancement, delayed washout pattern, and delayed plateau pattern, respectively. IBC and locally advanced breast cancer (LABC) remain two of the most aggressive forms breast cancer. Sometimes, it is difficult to identifying IBC and differentiating it from LABC in breast imaging. Despite being often grouped together, identifying IBC is very important, because IBC is a distinct clinical and pathological entity that requires distinct treatment from LABC. Girardi et al. (8) found a variety of statistically significant differences between the appearance of IBC and LABC at MRI. Skin changes (thickening, edema and enhancement) related to neoplastic involvement of the dermal lymphatics are suggestive of IBC than LABC (8910).
Non-Inflammatory Skin Involvement (Direct Skin Invasion, Satellite Skin Nodules)
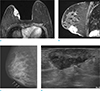
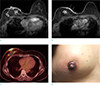
Superficial or locally advanced breast cancers can directly extend to the breast skin, usually causing skin thickening, focal (Fig. 3) or diffuse (Fig. 4), or multiple nodules (Fig. 5), even ulceration (Fig. 6) or fungating masses. In some cases, breast cancer with skin involvement by the indirect process, such as ipsilateral satellite skin nodules are seen on breast MRI (Fig. 7).
However, some superficial breast malignancies without direct skin invasion may cause edema or inflammation of the overlying skin, which is secondary change due to lymphatics or venous obstruction. The superficial malignancies, arising at ductal epithelium located just deep to the dermis, can be mistaken for malignant dermal involvement (1). In these cases, radiologist must be careful to avoid the misdiagnosis, but it is, often almost impossible. According to the current edition of the American Joint Committee on Cancer (AJCC) TNM staging system, non-inflammatory breast cancer with direct extension to the skin are classified as T4b lesions, the most advanced locoregional extent (stage IIIB). Undoubtedly, these findings were defined as grave prognostic factor for a long time (1112). Several systematic studies have reported widely differing prognostic and therapeutic implications in to these non-inflammatory breast cancer and they proposed the revision of TNM staging that would classify these tumors based on their tumor size and lymph node status (1314151617).
Local Tumor Recurrence with Skin Nodule
Locoregional tumor recurrence may occur in the breast skin rarely. Recurrence may involve the skin by means of (a) invasion along the Cooper ligaments to the retinacula cutis attachment points at the dermis, or (b) involvement of the lymphatic channels draining to the skin (18). Early detection of skin recurrence is crucial, because it has been shown to be a predictor for distant metastases, which is a poorer prognosis than other local recurrence. However, detection of early recurrence is difficult, because of background of treatment changes due to radiotherapy and/or surgery. The skin is difficult area to assess using mammography or ultrasonography, MRI may be the problem solving tool for early detection of skin recurrence (19202122). On MRI, focal and nodular enhancement or increased skin thickening are correlated with histology demonstrating tumor recurrence (Fig. 8), whereas linear, diffuse, or smooth enhancement is correlated with benign postoperative change (21). Most recurrences will occur in the quadrant of the original tumor, so focused clinical breast examination and imaging studies may provide earlier detection (23). When the findings are vague, pathologic confirmation should not be hesitated.
Other Malignancies
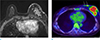
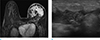
Other malignant diseases can involve breast skin are angiosarcoma, dermatofibrosarcoma protuberans, melanoma and non-breast metastasis. Angiosarcomas are rare tumors of endovascular origin and they are classified into primary and secondary groups. Radiation induced secondary angiosarcomas can affect breast cancer patient with history of radiotherapy following breast conserving surgery and their average latency period reported as 6-12.5 years. They are difficult to diagnose due to their rarity, benign appearance and difficulty in differentiation from radiation induced skin change (242526). On MRI, cutaneous angiosarcomas are shown as small enhancing skin lesions at irradiated site with varying kinetic patterns (27). Cutaneous metastasis is a relatively uncommon manifestation of breast malignancy. Frequent primary sites of cutaneous metastasis are originated from the lung, gastrointestinal, ovary and skin (melanomas). Lymphoma and leukemia also involve the breast skin (28). Most of the times it occurs late in the course of the disease, so the prognosis for patients with cutaneous metastasis is usually poor. On MRI, the cutaneous metastatic lesions are usually focal or diffuse skin thickening, but they often mimicking inflammatory cancer (29) (Fig. 9). Primary or secondary lymphoma may involve breast skin. T-cell lymphoma, especially subcutaneous panniculitis-like T-cell or peripheral T-cell lymphoma, preferentially infiltrate the subcutaneous tissue (3031). On MRI, irregular masses with a rim or heterogeneous enhancement in the subcutis may be present (32) (Figs. 10,11).
Nonmalignant Skin Involvement
Mastitis and Abscess
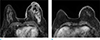
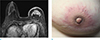
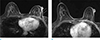
Mastitis may occur in the puerperal or non-puerperal state. The most common causative organisms are staphylococcus and streptococcus, although tuberculosis may sometimes be encountered. Clinically, these patients may present with a focal area of tenderness with associated erythema and induration (3334). Ultrasonography is very useful for evaluation inflammatory parenchymal and cutaneous change and detecting breast abscess, complications of mastitis. However, if there is no association of mastitis and abscess with pregnancy and lactation, or if there is inadequate resolution after antibiotic therapy, then ultrasonography-guided biopsy or MRI are useful to exclude inflammatory breast cancer. Acute mastitis shows overlapping imaging features with IBC (Figs. 12,13,14), however the combination of multiple dynamic and morphological criteria seems to have the potential for a differential diagnosis. The main location of acute mastitis was subareolar, whereas IBC are more often located centrally or dorsally. The following morphologic criteria, punched-out sign, T2-hypointensity of masses, blooming sign, infiltration of pectoralis major muscles, perifocal, prepectoral and intramuscular edema, is more often seen in IBC. The definition of punched-out sign, a reliable indicator for the lymphatic infiltration of the skin, is accentuated nodular enhancement of the skin occurring at fast in time, compared to surrounding normal skin (35). Nevertheless, if any diagnosis doubt exits, a histological verification is mandatory.
Chronic Granulomatous Mastitis
Chronic granulomatous mastitis is a very rare inflammatory disease of an unknown origin that can clinically and radiologically mimic infectious and malignant breast condition. This disease usually affects women of childbearing age or those with a history of oral contraceptive use. It is pathologically characterized by chronic granulomatous inflammation of the lobules without caseous necrosis or evidence of microorganism. The diagnosis of granulomatous mastitis is based on excluding other granulomatous reactions such as tuberculosis (363738). Although there are no radiologic pathognomonic findings specific to this entity, there is a few MRI characteristics can help differential diagnosis. MRI findings of peripherally located ring-enhancing lesions can suggest of chronic granulomatous mastitis (Fig. 15). The condition may respond to antibiotics and oral steroids, and surgery is also performed for disease control. The prognosis is often good, but local recurrence has been reported (39).
Edema
Breast edema can be caused by a variety of pathologic processes of benign or malignant disease, as a result of a tumor in the dermal lymphatics of the breast, lymphatic congestion caused by the breast, lymphatic drainage obstruction, or by systemic condition such as congestive heart failure and nephritis syndrome. Bilateral breast edema has mostly been reported in systemic problems. Mechanical problems such as obstruction due to lymph node enlargement (Fig. 16), subclavian vein occlusion, and especially arteriovenous hemodialysis complications, may cause unilateral breast edema (40).
Iatrogenic Change
As recently oncologic and plastic surgeries, core needle biopsies, mammotome procedure of the breast have increased, radiologist must cultivate an understanding of expected post-treatment imaging features and be able to differentiate these changes from suspicious breast lesions.
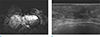
Recognizing the normal chronological imaging findings after breast conserving treatment with followed radiation change is important to minimize unnecessary recall or diagnostic work up. Focal skin thickening and/or enhancement, edema is commonly seen in the immediate postoperative period, but these imaging findings should be resolved with time (Fig. 17). These changes should not be interpreted as recurrent or remnant tumor involvement. After followed radiation therapy, diffuse or patchy skin enhancement and thickening, which correspond with radiation field, becomes more commonly (Fig. 18). The skin thickening seen on MRI of the breast correlated with histological thickening of the dermis by increased connective tissue and edema, and these changes presumably reflect radiation-induced inflammation and fibrosis (21). Skin enhancement is most often seen during the first 18 months after treatment, in some patients, residual faint enhancement may persist for several years (41). High-intensity focused ultrasound (HIFU) ablation is a rarely performed application for treatment of early-stage breast cancer, not a conventional treatment regimen for breast cancer. HIFU induces a temperature elevation and the tissue can be thermally destroyed by sonic energy (42), so one of its complications is skin burn (Fig. 19). These days, diverse reconstructive and cosmetic breast surgeries have evolved, familiarity with their imaging characteristics is essential for radiologic interpretation (Fig. 20). When equipped with an understanding of breast surgery techniques and their expected complications, radiologists may be able to differentiate normal postoperative changes from malignancy at imaging of these patients.
Trauma Related Change
Fat necrosis may result from accidental trauma is a relatively common benign entity in the breast. The inciting event on breast is often related to blunt trauma, such as motor vehicle crash and seat-belt injury. Fat necrosis has various appearances on MRI, typically benign to worrisome for malignancy; depend on the intensity of the inflammatory process. Because of its superficial location, some cases are associated with adjacent skin change, for instance bruise, edema, tethering or dimpling (43). These changes are shown as skin thickening and enhancement on breast MRI (Fig. 21). Eliciting the history of a traumatic event can be helpful in making the diagnosis of fat necrosis. Sometimes, fat necrosis may mimic breast cancer or concomitant breast cancer may be present, radiologist should be careful not to jump to conclusion.
Other Benign Disease
The most common dermal masses encountered by breast imagers are dermal cysts, specifically epidermal inclusion cysts and sebaceous cysts. Other common masses involving the hypodermal lesions are including lipoma, angiolipoma, hemangioma and thromobosed vessel (44). In addition, other dermatologic lesions could cause nonspecific skin thickening. Little study has been devoted to the appearance of these superficial lesions, because of they are not indication of MRI, but encountered at breast MRI incidentally. According to one of the few reports on the MRI appearance of dermal cysts, epidermal cyst, which is most common epithelial cyst of the breast, appear as a well-defined subcutaneous mass and isointense at T1-weighted imaging and heterogeneously hyperintense at T2-weighted imaging (45). These lesions may have peripheral rim enhancement that may even appear as solid internal progressive enhancement on postcontrast T1-weighted images, a finding that may be secondary to volume averaging. Recognizing the typical extension of the mass into the dermis can help make the correct diagnosis and usually localization of the lesions is more accurate at ultrasonography than MRI (1).
In conclusion, many conditions can involve the skin on breast MRI. Unfortunately, the skin lesions on breast MRI have been ignored because of the decreased spatial resolution of MRI. But, MRI finding preceded the patient's clinical evaluation and was the first change for detection of the abnormality. The radiologist must be familiar with various spectrum of cutaneous lesion. A high index of suspicion, careful patient evaluation and adequate biopsy tissue for pathologic diagnosis is mandatory for accurate diagnosis.










 XML Download
XML Download