

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Osteoid osteoma is a benign osteoblastic bone tumor that is usually encountered in adolescent and young adult males (1). The typical findings of osteoid osteoma in a long tubular bone are the presence of a small, well-defined radiolucent lesion with or without mineralization within the cortex, associated with cortical thickening and reactive sclerosis (2). Osteoid osteomas can be categorized according to its location in the bone; subperiosteal, intracortical, endosteal, or intramedullary (2). Subperiosteal form may produce atypical radiological features, and thus, in more than half of reported cases, the first diagnosis was wrong (3).
Few reports have been issued on subperiosteal osteoid osteoma, and the majority of reported images are radiographs or gross photographs. Here, we describe an unusual case of subperiosteal osteoid osteoma without reactive cortical thickening occurring in the distal femur and its radiographic, computed tomography (CT), ultrasonographic (US) and magnetic resonance imaging (MRI) characteristics.
CASE REPORT
A 19-year-old man presented with a 4-month history of pain in the posterolateral portion of the right knee. He complained of limited movement of the right knee joint and exacerbation of pain after sitting for a long time or bending the right knee. However, he had no difficulty in walking and did not complain of pain at night. The patient had no history of previous trauma, did not perform unusual or demanding activities, and had no systemic symptoms or lost weight.
On physical examination, the patient was able to fully extend his right knee, but flexion of > 120 degree was limited by severe pain. There was no focal tenderness, palpable mass or deformity over the posterolateral aspect of the right knee. Laboratory results were normal. Radiography of the right knee performed at initial visit showed faint calcification adjacent to the superior cortex of the lateral femoral condyle with focal, smooth erosion at the distal femur. No cortical sclerosis or thickening was evident (Fig. 1).
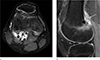
MR imaging of the right knee was performed 7 days after the radiography evaluation. It showed extensive bone marrow and soft tissue edema in the lateral femoral condyle on fat-suppressed T2-weighted and fat-suppressed proton-density images. And a small, round nodular lesion with low signal intensity at the extra-cortical, subperiosteal area was seen adjacent to the insertion site of the lateral head of the gastrocnemius muscle. Also elevated periosteum was noted as low signal intensity line on axial and sagittal T2-weighted image, so the lesion was thought to be in subperiosteal area (Fig. 2).
Since the presence of calcification adjacent to the muscle insertion site and extensive surrounding soft tissue edema, we first considered the possibility of acute phase hydroxyapatite deposition disease (HADD). The patient took nonsteroidal anti-inflammatory drugs (NSAIDs) for conservative therapy, but continued to complain of unchanged pain and discomfort of the right knee.
A CT scan was obtained about 3 months after conservative therapy. It showed a small nodular lesion with calcification located at the subperiosteal area causing smooth erosion of adjacent cortex without cortical thickening or periosteal reaction (Fig. 3a).
A bone scan revealed increased uptake of isotope at the right lateral femoral condyle (Fig. 3b) at about the same time.
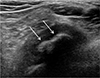
We decided to perform US-guided aspiration and to inject a mixture of steroid and lidocaine to exclude the possibility of HADD. However, under lidocaine local anesthesia, aspiration or biopsy of the calcified lesion was not possible, because the patient complained of intolerable pain when the needle was located in the lesion, and thus, we only injected the mixture (Fig. 4). The patient did not respond well to conservative therapy and complained persisting pain for about 5 months. To obtain a correct diagnosis, US-guided partial excision of the lesion was performed using a pituitary forceps through a small incision under spinal epidural anesthesia. Grossly, the resected specimen was a firm, lobulated, red-colored mass of diameter 0.5 cm (Fig. 5). Microscopically, the lesion was composed of trabeculae of woven bone lined with osteoblastic rimming and showed a mild to moderate proliferation of spindle cells that fill intertrabecular spaces (Fig. 6). These findings were diagnostic for osteoid osteoma.
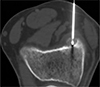
Curative treatment was performed by percutaneously CT-guided radiofrequency ablation (RFA) (Fig. 7), and one month later movement of the right knee was uninhibited and the pain had completely subsided.
DISCUSSION
Osteoid osteoma accounts for about 5% of all bone tumors and 11% of benign bone tumors (4). The majority of those affected are young and approximately one-half of patients are in the 2nd decade of life at presentation (5), as was the case for our patient. They may occur in any bone, but predominantly occur in the appendicular skeleton (4). In over 50% of cases, the lesions centered on the cortex of femoral and tibial diaphysis (6). In our case, the nidus was located in the supracondylar subperiosteal area of the femur. On axial fat-suppressed T2-weighted image, periosteal elevation was noted, so the lesion's location was thought to subperiosteal area (Fig. 2).
The radiographic findings of osteoid osteoma include a circular or ovoid cortical lucency representing the nidus (usually < 1.5 cm in diameter) with variable degrees of surrounding sclerosis. The center of the nidus is usually the most highly mineralized region, and degrees of mineralization vary (5). In our case, calcification largely composed the nidus.
The subperiosteal form has described as "round soft-tissue masses immediately adjacent to bone and as a rule, underlying bone reveals pressure atrophy or irregular bone resorption" (3). Osteoid osteomas arise in the subperiosteal region and subsequently become cortical or intramedullary (1).
The most common symptom is an unrelenting, sharp, boring pain, which often worsens at night and increases with activity, and is usually relieved by aspirin or other nonsteroidal anti-inflammatory drugs (5). Our patient had severe pain especially during flexion of the right knee, and thus, initially the clinician suspected a meniscal tear after physical examination, because the symptoms were differed from those typical of osteoid osteoma.
CT is the best modality for visualizing the nidus, because MR imaging sometimes fails to detect small nidi (7). It generally provides characterization of both the nidus and surrounding cortical sclerosis (5). However, CT may fail to prompt diagnosis when the nidus is in a cancellous location, due to a lack of perinidal density alteration (4). In our case, the calcification of the nidus was well depicted on CT, but a diagnosis of osteoid osteoma was not well made because of the absence of surrounding cortical thickening and an unusual location.
MR imaging demonstrates cortical involvement, intramedullary, and soft tissue spread, and thus, can be a valuable tool for tumor staging. Furthermore, MR imaging is excellent at detecting niduses of intra-articular lesions (4). In our case, the location of the nidus and extensive bone marrow edema were well demonstrated. Elevated periosteum overlying the nidus was detected as low signal intensity line on T2-weighted image, we could consider the lesion's location as subperiosteal. The nidus showed low signal intensity on all sequences due to calcification. Also extensive soft tissue edema and mass effect were noted around the lateral head of the gastrocnemius muscle. These findings may be explained by the combined subtendinous lateral gastrocnemius bursitis, and probably associated with the unusual image findings and clinical symptoms.
If no reactive bone is apparent, the nidus may be difficult to detect and radionuclide scans may be helpful for identifying the lesion. Increased Tc-99m uptake seldom reveals a local hot spot, but is usually diffuse and results from reactive hyperemia and associated synovitis (3). In our case, bone scan showed increased uptake at the right femoral condyle, but this finding was non-specific.
Osteoid osteomas can be treated conservatively with nonsteroidal anti-inflammatory drugs because they may undergo spontaneous regression after several years. However, when the patient keeps complaining of severe symptoms despite a trial of NSAIDs, complete surgical resection is the classic treatment of choice (4).
Recent technical development of RFA allow safe, effective ablation of osteoid osteoma. And RFA was preferred because of shorter hospital stay and shorter recovery time (6). CT-guided radiofrequency thermal ablation should be attempted only when a definite nidus is identified on CT scan. RFA and open surgical treatment have equivalent treatment outcomes (6). In our case, the patient strongly refused invasive open surgery so we first performed US-guided percutaneous partial excision using pituitary forceps with minimal incision for pathologic diagnosis. The lesion was confirmed as osteoid osteoma, we performed RFA for curative treatment.
In summary, osteoid osteoma in a common location and typical findings is easily diagnosed. However, the correct diagnosis of an osteoid osteoma may be challenging when it arises from an unusual location, such as a subperiosteal area and is not associated with reactive bone changes, such as, cortical thickening or sclerosis. We concluded that awareness of the imaging features of subperiosteal osteoid osteoma will aid radiologist to make its differential diagnosis.




 XML Download
XML Download