

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In the past, leukemic involvement of central nervous system (CNS) was uncommon because leukemia rapidly progressed and was often fatal. However, the frequency of leukemic involvement of the CNS has increased due to prolonged survival associated with development of treatment (1234). Leukemic involvement of the eye may be present over the optic nerve, orbit, uveal, choroidal or retinal layer. While leukemic infiltration of the orbit is common, leukemic involvement of the optic nerve is relatively rare. Nevertheless, leukemic infiltration of the optic nerve is clinically significant because it may be an isolated manifestation of leukemia relapse and local treatment such as radiation therapy may be required (45).
When the enhancing optic nerve thickening in leukemic patients is seen on magnetic resonance imaging (MRI), this finding may suggest leukemic involvement of optic nerve (6). But, the possibility of optic neuritis cannot be excluded. Leukemic infiltration of optic nerve and optic neuritis has similar imaging and clinical findings, and it is difficult to make a differentiation between these only based on imaging finding. Therefore, the additional examinations (such as cerebrospinal fluid [CSF] or bone marrow [BM] study) are recommended and helpful for accurate diagnosis and proper management of patients with history of leukemia. Because the treatments of leukemic infiltration of optic nerve and optic neuritis are critically different, the differentiation between two diseases is very important.
MATERIALS AND METHODS
Our study was approved by our Institutional Review Boards. We retrospectively reviewed the brain and orbit MRI of 7 patients with leukemia diagnosed with leukemic infiltration of optic nerve (n = 5) and optic neuritis (n = 2) in our institution between July 2006 and August 2015. The diagnosis of leukemic infiltration of optic nerve and optic neuritis was established on the basis of the combination of histologic evidence of CSF involvement by leukemia, treatment response, and progress of underlying leukemia.
Using both 1.5T system (Signa Excite; GE Healthcare, Madison, WI, USA) and 3.0T system (MagnetomVerio; Siemens Medical Solutions, Erlangen, Germany), we obtained various sequence imagings, including T1-weighted, fat-suppressed T1-weighted, fat-suppressed T2-weighted, and contrast-enhanced fat-suppressed T1-weighted images. All MR images were retrospectively reviewed by 2 radiologists blinded to the histologic diagnosis and decisions were reached by consensus. Imaging features included the presence of perineural enhancement and thickening of optic nerve and its degree, signal intensity, laterality (unilateral/bilateral), intraconal fat infiltration and its degree, and associated CNS abnormalities such as accentuated leptomeningeal enhancement or chloroma.
The medical records including sex, age at diagnosis, symptom, disease status of leukemia at diagnosis of optic nerve lesion, treatment and outcome were carefully reviewed. The results of CSF studies and BM biopsies were also reviewed.
RESULTS
Clinical Data
Table 1 shows clinical findings of 7 cases. Of the 7 patients, 5 were men and 2 were women between 6 and 60 years of age (mean age, 21 years). The patients had one of three types of leukemia, including 5 cases of acute lymphoblastic leukemia (ALL), 1 case of acute myelogenous leukemia (AML), and 1 case of chronic myelogenous leukemia (CML). The disease status of patients were first complete remission (n = 2), second complete remission (n = 3), refractory state (n = 1) and 1 of 7 patients was being treated with imatinib at the time of presentation. Patient symptoms included only decreased visual acuity (n = 2) or decreased visual acuity with foreign body sensation (n = 1) or fever (n = 1), visual field defect (n = 1), diplopia (n = 1), and painful swelling of the eye (n = 1).
Imaging Findings
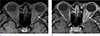
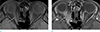
The MR imaging features of 7 cases are summarized in the Table 2. Of 5 leukemic infiltration of optic nerve, 4 cases showed unilateral involvement and 1 case showed bilateral involvement (Figs. 1,2,3). All 2 optic neuritis lesions showed unilateral involvement (Fig. 4). All 7 cases displayed enhancing thickening of optic nerve, with variable degree of enhancement and thickening without significant difference between two groups. All cases also showed variable intraconal fat infiltration. The signal intensity of leukemic infiltration of optic nerve and optic neuritis on unenhanced MR imaging was similar, and all lesions showed low signal intensity to isointensity on T1-weighted images and high signal intensity on T2-weighted images. After gadoliniumbased contrast administration, all 7 cases showed perineural enhancement. Of the 5 leukemic infiltrations of optic nerve, 2 cases showed imaging findings consistent with leukemia including prominent leptomeningeal enhancement (n = 1) and chloroma (n = 1) (Fig. 2c and 3d).
Histologic Findings, Treatment and Outcome
The leukemic infiltration of optic nerve was diagnosed by histologic evidence of CSF study and BM biopsy. Of the 5 leukemic infiltrations of optic nerve, according to the order in Table 1, case number 1, 4, and 5 showed positive CSF study for leukemia relapse. Case number 2 of the 5 leukemic infiltrations of optic nerve showed normal CSF study and positive BM biopsy for leukemia relapse. Case number 3 of the 5 leukemic infiltrations of optic nerve showed positive results on both CSF study and BM biopsy for leukemia relapse. In these cases, the diagnosis of leukemic infiltration of optic nerve was proposed, and chemotherapy or radiation therapy or cytoreduction was started. In case number 1 and 4 of 5 leukemic infiltrations of optic nerve, follow-up MRI was not performed, but follow-up CSF study showed regression of leukemia involvement 8 and 30 days after initiation of anti-leukemic therapy. In these cases, one patient died due to gastrointestinal bleeding and pulmonary hemorrhage after 3 months; another patient died of pneumonia, which occurred during chemotherapy for fourth CNS relapse after 4 years. In a case number 5 of the 5 leukemic infiltrations of optic nerve, follow-up MRI and CSF study showed regression of leukemia involvement 2-3 months after the initiation of anti-leukemic therapy. This patient died due to pulmonary hemorrhage and respiration failure after 3 years. In a case number 2 of the 5 leukemic infiltrations of optic nerve, the initial CSF study was found to be negative for leukemic involvement but subsequent BM biopsy revealed leukemic involvement. Follow-up MRI showed regression of leukemia involvement 1 month after the initiation of anti-leukemic therapy, and further follow-up BM biopsy showed leukemic involvement. The patient was transferred to another hospital and there was no further follow-up of the patient. In a case number 3 of the 5 leukemic infiltrations of optic nerve, follow-up MRI and CSF study showed regression of leukemic involvement 2 weeks after the initiation of anti-leukemic therapy. He had achieved complete remission and he has undertaken follow-up examination.
However, 3 patients (case number 1, 4, and 5) of 5 the leukemic infiltrations of optic nerve died within 3 years after this recurrence, one (case number 2) of the rest patients was transferred to another hospital and another patient (case number 3) has been in complete remission for 8 years after this recurrence.
In 1 case (case number 7) of 2 patients with optic neuritis, CSF study and BM biopsy was not performed. And another case (case number 6) showed normal CSF study. In these cases, the clinical diagnosis of optic neuritis had been proposed, and pulse steroid therapy was started. The symptoms and signs were improved 10 and 14 days after undertaking steroid therapy and they had undertaken maintenance therapy.
DISCUSSION
The thickening and enhancement of optic nerve in patients with underlying leukemia should be suspected of leukemic infiltration of optic nerve and should be differentiated from optic neuritis. The leukemic infiltration of optic nerve and optic neuritis has comparable symptoms and signs, similar to that observed in our cases. The leukemic infiltration of optic nerve is also more common in children than in adults (68). In our series, all 5 patients with leukemic infiltration of optic nerve had previous history of ALL, raising the possibility that the leukemic infiltration of optic nerve occurs most frequently in patients with ALL (6).
The optic nerve is one of leukemia relapse sites because the chemotherapeutic drugs cannot penetrate blood-brain barrier and the invasion of leukemic cells in the small optic canal can interfere with the flow of CSF. In rarer cases, the optic nerve is the only initial manifestation site of leukemia relapse in a patient with prior complete remission (6711). Similarly, in our series, 4 of 5 patients with leukemic infiltration of optic nerve achieved complete remission and had no previous history of central nervous system involvement.
Due to their low prevalence, only a few literatures have addressed the MR imaging findings of leukemic infiltration of optic nerve (68910111213). A search of the literature in English showed 6 cases of leukemic infiltrations of optic nerve (Table 3). MR imaging finding of the leukemic infiltration of optic nerve is thickening of the optic nerve with enhancement (68910111213). Enhancing optic nerve thickening is also noted in patients with optic neuritis, however, no case of optic neuritis in leukemic patient has been reported yet. In our results, all 2 patients with optic neuritis and 5 patients with leukemic infiltration of optic nerve show variable enhancement and thickening of optic nerve with variable perilesional intraconal fat infiltration on MRI, without significant difference between two groups. However, MR imaging findings of associated other CNS involvement are helpful in distinguishing the leukemic infiltration of optic nerve from optic neuritis. In our series, 2 of the 5 patients with leukemic infiltration of optic nerve showed leptomeningeal enhancement or intracranial chloroma on MRI.
In 5 patients with leukemic infiltration of optic nerve, follow-up MRI or CSF studies showed regression of leukemic infiltration after receiving chemotherapy and radiation therapy, but 3 of the 5 patients died. In 2 patients with optic neuritis, their symptoms improved after receiving pulse steroid therapy and they had undertaken maintenance therapy with longer survival rate. This study has a limitation due to very small sample size and this is not enough to represent the overall entity. However, the treatment and prognosis of leukemic infiltration of optic nerve and optic neuritis are generally different (512). Thus it is important to differentiate them. Thus, future studies should increase the sample size and demonstrate helpful imaging and clinical findings in distinguishing the leukemic infiltration of optic nerve from optic neuritis.
In conclusion, enhancing optic nerve thickening is overlapped MR imaging findings between leukemic infiltration of optic nerve and optic neuritis. However, the most specific MR findings for CNS involvement of leukemia include leptomeningeal or parenchymal abnormalities. Then, our findings suggested that in patients with history of ALL (6), enhancing optic nerve thickening with associated CNS abnormality favor the diagnosis as leukemic infiltration of optic nerve. However, the possibility of optic neuritis cannot be excluded, therefore, CSF and BM biopsy are necessary for differentiation.





 XML Download
XML Download