This article has been
cited by other articles in ScienceCentral.
Abstract
Purpose
Operating room management is the serious and complex task for hospital managers and the common approach is to develop relevant standard operational procedures. From patient and staff safety perspective, operating room management should be well-studied and hospital should identify and address any potential risks. Simultaneous usage of different imaging and less-invasive treatment technologies demands strong management control.
Materials and Methods
We have formed the multidisciplinary expert panel (surgeons, anesthesiologists, radiologists, healthcare managers etc.) for hybrid theater management standard operational procedure development. On the first stage the general concept of hybrid room design and patient routing was developed. The second stage included the technical details discussion. For patient safety improvement we modified the Surgical Safety Check-list in accordance with potential MRI-related safety challenges and concerns.
Results
WHO Surgical Safety Checklist is a simple and easy-to use tool which includes three blocks of question (grouped by the surgery process). We have developed two additional blocks of questions for the intraoperative magnetic resonance investigation. It is very important to have a special detailed routing with a strong control of ferromagnetic devices and anesthesiology care.
Conclusion
High-energy MRI (1.5-3.0T) is characterized by potential influence on patient and staff safety in case of hybrid surgery. It is obvious to have a strong managerial control of ferromagnetic devices and anesthesiology care. Surgical Safety Checklist is the validated tool for improving patient safety. Modification and customization of this check-list potentially provides the opportunity for surgery processes improving.
Keywords: Hybrid operating room, Surgical safety checklist, Patient safety, Magnetic resonance imaging
INTRODUCTION
Operating room management is a serious and complex task for hospital managers and the common approach is to develop relevant standard operational procedures. From patient' and staff safety perspective operating room management should be well-studied and hospital should identify and address any potential risks. Implementation of standard validated tools, especially in safety-related area, is the obvious part of diagnostic and treatment processes management. Since 2008 WHO's (Safe surgery save lives) program was implemented worldwide and the Surgical Safety Checklist (SSCL) is the international standard validated tool for operating room management and the part of real clinical practice (
1). This program currently is covering more than 3900 hospitals in 122 countries; 25 countries declared this initiative as a national project (
2). Nowadays based on epidemiological studies, it is considered that SSCL usage significantly and reliably reduces mortality (from 1.5% to 0.8%) and postoperative complications rate (from 27.3 to 16.7 for 100 cases) (
345).
In case of hybrid operating theater with intraoperative magnetic resonance imaging (MRI) this management strategy looks like not only recommendation but a necessary condition and a standard for processes control. Simultaneous usage of different visualization and less-invasive treatment technologies are characterized by potential influence on patient safety. In general, MRI has a good safety profile, but there are some identified risks:
Displacement forces on ferromagnetic objects in the high-energy magnetic field,
Risks of thermal injury due to RF-induced heating,
Risk of MRI noise-related hearing impairment
US Regulatory Authorities (American Society for Testing and Materials [ASTM] and U.S. Food and Drug Administration [FDA]) defined that "MR Safe" as an item that poses no known hazard in all MRI environments. "MR Safe" items are non-conducting, non-metallic, and non-magnetic (
6). By the way, this definition covers just safety aspects, but not machine functioning and imaging quality influence. More broad and considerable with a lot of areas is "MR-compatible" term. Such that all components inside scanner room have been demonstrated (
7):
Not to pose any known hazards in its intended configuration (corresponding to the ASTM definition of MR Conditional),
Not to have its intended functions deteriorated by the MRI system,
Not to significantly affect the quality of the diagnostic information
According to these criteria the most part of the operating room equipment are MR-unsafe and MR-incompatible (surgical tools, operating table, ventilator, light sources, imaging systems, angiography devices etc.). This fact demands a precise hybrid theater design and planning and management processes standardization (
8). Intraoperative MRI in high-energy field (1.5-3.0T) followed with strong conditions for ferromagnetic and non-magnetic surgical tools control and accurate patient logistics and routing (
9). All MR-Unsafe equipment must have clear marking to avoid any risks. Anesthesiology care also is the important question in case of intraoperative MRI (
10). For vital functions monitoring and support a hospital needs to have the MR-compatible anesthesiology equipment (special ventilator, infusion pumps, pulse oximeters, catheters, needles etc.) (
8). White et al. (
8) suggest that modified surgical safety checklist is the applicable tool for the safety risks ensuring and allows the strong MR-related challenges control.
Hybrid surgery means a combination of conventional and endovascular interventions, thus a facility planning team needs to consider not only magnetic field but both MR-related, sterility, anesthesiology care and radiation-related aspects.
Therefore MRI-equipped hybrid room creating and functioning is a difficult and complex problem.
MATERIALS AND METHODS
For hybrid operating room management system development the multidisciplinary expert panel was established in 2015. Healthcare managers, surgeons, oncologists, radiologists, anesthesiologists, MRI technicians, engineers, architects and facility planning specialists, IT-staff, radiation safety specialist were taken on board.
On the first stage the risk minimization roadmap was developed. We have analyzed the existing decisions; surgery and intensive care units' plans; corridors and rooms zoning consider with magnetic field and potential radiofrequency induction; air-conditioning, ventilation, electrical, water and medical gases communications; MR-scanner placement and magnetic field power; operating table, C-arm and radiation safety, anesthesiology equipment and other medical devices placement. Each function's representative received the individual specific list of questions for discussion. Regular workshops were organized for potential risk assessment and risk avoiding and minimization plans/scenarios creation and implementation.
On the second stage of "Hybrid operating room management" the standard operational procedure was developed. It was a detailed description of intra hospital and intradepartmental (operating room - intensive care unit) patient routing; surgery room zoning with sterility and magnetic field conditions; algorithm for MR-compatible and MR-unsafe tools and medical devices usage, marking, registration and control.
SOP development and justification were facilitated due to our previous experience with C-arm and radiolucent table equipped hybrid room building and exploitation since 2013. During 2014-2016 we have performed 81 MR-guided intervention in operating room (direct tumor biopsies with different localization). Biopsies were conducted with special coils (for body tumors) or Leksell frames (for intracranial tumors) and non-magnetic needles with in-bore positioning control by high-field MRI (Siemens MAGNETOM Verio 3T, Erlangen, Germany). In 75 cases it was direct prostate biopsy (
Fig. 1), in 6 cases - stereotactic brain tumor biopsies (
Fig. 2). Thus MR-related safety challenges and MR-assisted invasive technologies management (with MR-compatibility, non-magnetic tools, operating room space zoning etc.) were not unexpected for us.
For patient intraoperative routing and adequate safety monitoring ensuring standard WHO surgical safety checklist was modified. SSCL includes three simple and easy-to-use blocks of questions, grouped by the surgery stages (
Fig. 3).
Before anesthesia introduction, medical staff need to identify the patient, surgery localization and type and assess anesthesiology risks and equipment. Before invasion (surgical, endoscopic or endovascular), surgeon, nurse and anesthesiologist prepare the surgery plan, sterility, equipment functioning assessment, highlight and prevent the risks. After surgery and before patient's moving into intensive care unit, medical staff should confirm the documentation records, histology marking, tools and expendables calculation and provide with short postoperative patient's management plan. Therefore, SSCL is covering all important surgery-related risks and potentially helps to avoid complications.
SSCL is the individual control tool for the concrete operation, the copy of list usually archived in the patient's medical records. All collected data typically used for surgical service efficacy analysis. Standard SSCL was implemented in our hospital since March 2015 for C-arm equipped hybrid theatre and currently all surgery is usually performed with this management system, but for MRI-equipped room this list was modified in accordance with magnetic field-related challenges and concerns.
RESULTS AND DISCUSSION
Currently two MR-scanner's placement concepts for hybrid surgery exist: the machine in the additional room (garage) with patients' moving during operation or sliding gantry (with ceiling rails). Both concepts have some advantages and restrictions but we have decided to avoid the movable scanner due to potential images' quality issues and sterility concerns. Therefore, we have concentrated on safely patients' routing. As a result of the expert panel discussion and local/international guidelines, legislation and scientific literature analysis we suggest the following statements for the MRI-equipped hybrid operating room design:
Clear color marking of magnetic field lines on the operating room floor (safe surgery is possible outside of 0,5 mT - 5 Gauss magnetic field power)
MR-scanner room separation with locked door and electronic controlled staff access
Clear and obvious marking for all MR-unsafe devices
Strong control for non-magnetic surgical tools (storage and sterilization in separate set, placement during surgery on separate color-marked table, calculation and accounting with records on the special lists)
Special color marks for equipment (green - MR-safe, yellow - MR-compatible, red - MR-unsafe) (Fig. 4). In general, color marks usually placed on patient's trolley (it should be MR-safe); ventilator and other anesthesiology devices (MR-compatible), non-magnetic surgery and biopsy tools in case of its usage in-bore (MR-compatible). All equipment into MRI room should be MR-safe or, at least, MR-compatible.
In case of endovascular interventions (stents placement, embolization etc.) it should be performed after MRI due to potential safety and image quality issues (just one exception - diagnostic angiography);
Strong continuing control for all surgery stages with modified surgical safety checklist.
Based on WHO SSCL, we have developed two additional blocks of questions for intraoperative magnetic resonance investigation (
Table 1). The first block is describing step-by-step actions, performed by surgeon, radiologist and anesthesiologist before intraoperative MRI - absence of magnetic tools and devices, sterility check, patient's switch to MR-compatible ventilation, scanner ready to use. The second block is needed for control processes after MRI - coil removal, ventilation switch to conventional machine, start of next surgery or intervention.
For our facility concept with separated MRI-room the anesthesiology care is the serious challenge. Conventional MR-unsafe ventilator's usage is prohibited within high-energy static magnetic field, therefore in MRI room special non-magnetic ventilator should be placed and the patient will be connected to it directly before investigation. MR-compatible ventilator should be placed in safe magnetic area to avoid imaging artifacts and to maintain adequate functioning (
Fig. 5). Thus the most important task is the adequate patient's preparation for switching from conventional to non-magnetic ventilation and to support vital functions during transportation and imaging procedure.
Historically, checklists were implemented for the first time for aviation safety and then spread for different areas, including medicine (
12). Modern operating room, especially a hybrid theater, equipped with different diagnostic imaging systems and invasive devices really may be compared with an aircraft and similar management tools implementation declared by many authors as a justified and helpful approach.
White et al. (
8) suggest not only to use checklists in daily practice, but to appoint a special person (usually radiologist) - Procedure Safety Officer - to control the safety protocol realization and to make records with SSCL. Soroka et al. (
13) also offer to appoint a physician as a manager, who will be responsible for the processes monitoring on the regular basis (or for the concrete operation). Childs and Bruch (
14), based on their intraoperative MRI experience, specified some important points - the detailed preparation for the diagnostic stage and safety protocol development are mandatory. In addition, the necessary part of hybrid surgery theater governance is the staff training (
15). All involved healthcare providers, technicians, managers should be trained regarding operational procedure, radiation and MRI safety aspects, risk minimization plans and emergency resolving.
Thus we would like to note that strong high-energy magnetic field risk assessment, adequate operating room space design, safety protocol development and implementation are helpful for surgery management optimization and complications avoiding. In general, surgical safety checklists, as a part of operating room management system, improving safety results. SSCL's adoption and modification is declared by World Health Organization as the positive practice.
In conclusion, intraoperative MRI characterized by the potential influence on patient and staff safety and demands a serious planning on the facility design stage. The optimal way is the involvement of a group of different specialists, including healthcare providers for the planning process. Operating space zoning with the MR-related safety challenges and controlled staff access is the important point. It is obvious to have a strong managerial control of ferromagnetic devices and anesthesiology care. Hybrid operating room management demands the special protocol (standard operational procedure) development and implementation. We support the practice of the Procedure Safety Officer appointment and strong staff training. Modified surgical safety checklist implementation for MRI-assisted surgery potentially may improve the operating room management and increase patient and staff safety.
Figures and Tables
Fig. 1
In-bore MR-guided prostate biopsy. Biopsy coil and non-magnetic needle positioning.
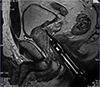
Fig. 2
Stereotactic brain tumor biopsy.

Fig. 3
In-bore MR-guided prostate biopsy. Biopsy coil and non-magnetic needle positioning.

Fig. 4
Color marks for equipment.

Fig. 5
MRI-equipped operating room blueprint.

Table 1
Additional Blocks of Questions for Intraoperative MRI

|
Before intraoperative MRI |
After intraoperative MRI |
|
Surgeon and nurse confirm: |
Radiologist confirm: |
|
- Imaging area |
- Magnetic resonance scanner turning off |
|
- Ferromagnetic tools and devices absence |
- Coil removal |
|
- Quantity of non-magnetic tools in the operating field |
|
|
Anesthesiologist confirm: |
Anesthesiologist confirm: |
|
- Patient’s readiness for transportation and switch to non-magnetic ventilator |
- Patient’s readiness for transportation and switch to standard ventilator |
|
- Start of ventilation by non-magnetic ventilator |
- Start of standard ventilation |
|
- Ferromagnetic devices absence |
|
|
Radiologist confirm: |
Surgeon and nurse confirm: |
|
- Coil placement |
- Non-magnetic devices quantity |
|
- Coil sterility |
- Start of next surgery stage |
|
- Staff absence |
|
|
- Magnetic resonance scanner turning on |
|
Acknowledgments
Authors would like to acknowledge Evgeny Pinelis, MD (Albert Einstein School of Medicine, NY, USA) for design contribution, risk minimization map development and validation, English checking as the professional editor.
References
1. Sivathasan N, Rakowski KR, Robertson BF, Vijayarajan L. The World Health Organization's 'Surgical Safety Checklist': should evidence-based initiatives be enforced in hospital policy? JRSM Short Rep. 2010; 1:40.
2. Conley DM, Singer SJ, Edmondson L, Berry WR, Gawande AA. Effective surgical safety checklist implementation. J Am Coll Surg. 2011; 212:873–879.
3. Haynes AB, Weiser TG, Berry WR, et al. A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med. 2009; 360:491–499.
4. de Vries EN, Prins HA, Crolla RM, et al. Effect of a comprehensive surgical safety system on patient outcomes. N Engl J Med. 2010; 363:1928–1937.
5. Neily J, Mills PD, Young-Xu Y, et al. Association between implementation of a medical team training program and surgical mortality. JAMA. 2010; 304:1693–1700.
6. Li G, Su H, Cole GA, et al. Robotic system for MRI-guided stereotactic neurosurgery. IEEE Trans Biomed Eng. 2015; 62:1077–1088.
7. Yu N, Gassert R, Riener R. Mutual interferences and design principles for mechatronic devices in magnetic resonance imaging. Int J Comput Assist Radiol Surg. 2011; 6:473–488.
8. White MJ, Thornton JS, Hawkes DJ, et al. Design, operation, and safety of single-room interventional MRI suites: practical experience from two centers. J Magn Reson Imaging. 2015; 41:34–43.
9. Porteous J. Intraoperative MRI: the challenges of providing a safe environment for patients and personnel. 201. ORNAC J. 2014; 32:12–14. 16–19. 22 passim
10. Henrichs B, Walsh RP. Intraoperative MRI for neurosurgical and general surgical interventions. Curr Opin Anaesthesiol. 2014; 27:448–452.
12. Helmreich RL. On error management: lessons from aviation. BMJ. 2000; 320:781–785.
13. Soroka VV, Andreichuk KA, Kechaeva EI, Postnov AA, Kagachev PN. Hybrid operating room: a new horizon in cardiovascular surgery. Angiol Sosud Khir. 2011; 17:93–101.
14. Childs S, Bruch P. Successful management of risk in the hybrid OR. AORN J. 2015; 101:223–234. quiz 235-227.
15. Hemingway M, Kilfoyle M. Safety planning for intraoperative magnetic resonance imaging. AORN J. 2013; 98:508–524.


 PDF
PDF ePub
ePub Citation
Citation Print
Print


 XML Download
XML Download