

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Tenosynovial giant cell tumor is a part of the spectrum of benign synovial proliferative lesions. The patients are usually adults and the peak incidence is the third to the fifth decades of life. The majority of these lesions occur in the hands and wrists. The characteristic MR imaging finding of tenosynovial giant cell tumor is hypointense signal intensity seen on T1- and T2-weighted images. Osseous abnormalities associated with tenosynovial giant cell tumor include pressure erosion, cystic change and degenerative change (1). However, severe bone involvement by tenosynovial giant cell tumor has infrequently been reported. This case report intends to describe tenosynovial giant cell tumor showing severe bone erosion and to review the literatures regarding bone lesions and their clinical significance such as the relationship between bone erosion and prognosis of tenosynovial giant cell tumor.
CASE REPORT
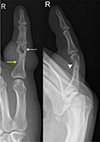
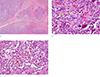
A 46-year-old man presented with a mass in the proximal phalanx level of his right fifth finger. The mass lesion was first detected as soft-tissue swelling 15 months previously, and the patient explained that the mass was slowly growing. He had experienced discomfort, such as a pulling sense of his skin, for two weeks before visiting the hospital. He had no history of trauma or cancer. On physical examination, there was no remarkable finding except for the soft-tissue mass in his right fifth finger, and he complained of no pain or tenderness in this finger. The mass was firm and showed a lobulated contour. The function of the PIP joint of the fifth finger was normal. Plain radiographs showed a soft-tissue mass showing a bulging contour in the proximal phalanx level of his right fifth finger. And intramedullary and cortical cystic lesions together with cortical erosion and trabeculation were detected. However, definite cortical perforation or cortical destruction was not found (Fig. 1). On MR imaging, the mass revealed an irregular margin, and circumferential growth surrounding the flexor digitorum tendon. Bone involvement by a soft-tissue mass and its intraosseous extension, when seen on MR images, is more aggressive than bone lesions seen on plain radiographs. The mass showed slightly hyperintense signal intensity to muscle on T1- and T2-weighted images (Fig. 2). However, dark signal intensity on T2-weighted images was seen in the periphery of the mass (Fig. 2b). A bone scan showed a mild increase in uptake in the right fifth finger (Fig. 3). According to these features, we suspected a tenosynovial giant cell tumor as this is a common benign soft-tissue tumor in the hand and shows slow growth. The differential diagnosis included fibroma and the possibility of desmoid-type fibromatosis and soft tissue sarcoma due to the severe bone invasion seen on MR images. Eventually, radical excision of the mass was performed. According to the intraoperative findings, the tumor had a yellowish color, a multi-lobulated contour, circumferential growth surrounding the proximal phalanx of the right fifth finger, and an ill-defined margin with adjacent bone and soft tissue. On pathologic examination, the tumor was proven to be a tenosynovial giant cell tumor which consisted of a polymorphous population of mononuclear stromal cells with small, round, spindle, rentiform nuclei, epithelioid macrophages with abundant eosinophilic cytoplasm, and vesicular nuclei and osteoclast-like giant cells (Fig. 4).
DISCUSSION
Tenosynovial giant cell tumor, also termed nodular tenosynovitis, is a benign, synovial, proliferative disease and one of the most common soft-tissue masses in the hand. Most patients are adults and present with a slowly growing and painless soft tissue-mass. The mass is mobile under the skin, although it is attached to deeper structures. The histological finding includes synovial proliferation with scattered multinucleated giant cells, macrophages, fibroblasts, and xanthoma cells (1). Varying amounts of hemosiderin may be observed. Because of the hemosiderin contents, tenosynovial giant cell tumor shows decreased signal intensity on both T1- and T2-weighted images. These features may be useful for differentiating it from other soft-tissue tumors occurring in the hand (2).
From the review of previous reports, bone lesion and intraosseous invasion by tenosynovial giant cell tumor have not been given attention and the focus was on the imaging findings of plain radiographs in the published reports. On the radiographs of patients with tenosynovial giant cell tumor, osseous abnormalities included pressure erosions, cystic change, and degenerative change (1). Uriburu et al. (3) reported 15 patients with tenosynovial giant cell tumor showing intraosseous growth in the digits. The most frequently involved site was phalanges among the affected digits. Typical radiographic findings include intraosseous lucency, cortical thinning, a subtle rim of perilesional bone sclerosis, and a coarse rim. Intraosseous lucency was seen in all of the patients. And in six patients, the bone lesion was a multilocular lesion in which the locule was separated from adjoining bones by normal or condensed bone trabeculae. De Schepper et al. (4) reported six patients with tenosynovial giant cell tumor. Three of these six patients showed a sharply marginated cortical lesion, one had a cortical defect and pressure erosion and two had an expansile intramedullary lesion of geographic destruction.
The differential diagnosis of tenosynovial giant cell tumor in the finger can include any soft tissue mass with low signal intensity seen on both T1- and T2-weighted images. Typical tenosynovial giant cell tumor shows a similar imaging finding with fibroma of the tendon sheath. However, fibroma of the tendon sheath is a rare benign tumor and bone involvement secondary to remodeling or extrinsic erosion in the finger is very uncommon (5). Atypical tenosynovial giant cell tumor with severe bone erosion can be differentiated from demoid-type fibromatosis and soft tissue sarcoma such as fibrosarcoma and undifferentiated sarcoma. Desmoid-type fibromatoses are usually intermuscular masses of deep soft tissue and characteristically grow along fascial planes (6). And in general, soft tissue sarcomas in the hand show an ill-defined margin, relatively large size, and heterogeneous signal intensity on T2-weighted images (7). However, actually distinguishing between a tenosynovial giant cell tumor and a soft tissue sarcoma using imaging finding is difficult.
Because an intraosseous bone lesion of tenosynovial giant cell tumor is related to the tumor recurrence and prognosis, complete resection of tenosynovial giant cell tumor is very critical for treating the disease and incomplete resection due to bone erosion or invasion by the tumor may be a significant risk factor for local tumor recurrence in the hand (8). Jalgaonkar et al. (9) recommended that curettage of the bone should be done in patients with osseous erosion in order to prevent recurrence. And Lu et al. (10) reported the case of artificial finger joint replacement in a patient with tenosynovial giant cell tumor as well as bone destruction that did not show complications such as tumor recurrence or joint dislocation. Therefore, diagnostic imaging, including radiography, CT and MRI, are all important for patients with tenosynovial giant cell tumor showing severe bone erosion. And from our review of past reports, CT and MRI have an important role for clearly demonstrating the intraosseous component of tenosynovial giant cell tumor. Through review of our case we can learn imaging finding of tenosynovial giant cell tumor with severe bone erosion and the application of imaging findings to clinical practice.


 XML Download
XML Download