

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Brain metastases are the most common intracranial tumors, and this rapidly growing incidence is likely due to the growing effectiveness of therapies for primary malignant tumors and improved detection with new CNS imaging modalities. Brain metastases occur in 20-40% of patients with systemic cancer (1, 2). The diagnosis and determination of the number of brain metastases influence staging as well as therapy (3). The median survival time of patients with one or only two brain metastases in non-eloquent brain areas can be prolonged up to 14 months by stereotactic radiotherapy or by operation followed by radiotherapy (3, 4). Multiple or inoperable brain metastases are mostly decisive for the prognosis of metastatic cancer. In patients with multiple brain metastases, the therapeutic possibilities are currently limited to whole-brain radiation and/or chemotherapy without surgery. The resulting median survival time rarely exceeds 6 months. Hence, the detection and identification of brain metastases with respect to number, size, and location are indispensable for optimal therapeutic management.
MRI with contrast administration has been shown to be the most sensitive imaging modality for detecting brain metastases noninvasively (5, 6, 7). Several strategies to improve the detection rate of brain metastases by MRI have been reported: the use of a higher dose of contrast agent (8, 9), the use of magnetization transfer contrast (10), and MR examinations with higher field strength (11, 12). With an increased magnetic field, the signal-to-noise ratio (SNR) increases almost linearly. Hence, ultra high field MRI allows improvement of the spatial resolution without sacrificing the SNR and contrast-to-noise ratio compared to MRI at lower field strengths (13, 14). Ultra high field MR whole-body scanners at 7.0T to 9.4T are currently being tested for clinical application in humans. Several studies have already proved the superior sensitivity and specificity of 3.0T versus 1.5T MR systems for imaging brain tumors and brain metastases (15, 16, 17). 3.0T MRI allows a reduction in the contrast media dose to half of the standard dose while still rendering similar contrast compared to 1.5T (15, 17).
The purpose of this study was to evaluate depiction of brain metastases after intravenous administration of the clinically established single-dose of gadolinium-based contrast media at 7.0T compared to double-dose 1.5T.
MATERIALS AND METHODS
Patients
We received the permission from the Korean Food and Drug Administration and the Institutional Review Board of Seoul National University Hospital and the Neuroscience Research Institute of Gacheon Medical Center, and we obtained written informed consent from all subjects. Adult (>20-year-old) patients with brain metastasis of histologically proven primary tumors at 1.5T MRI were included. Prior to enrollment, all study participants were informed of the scientific nature of 7.0T MR examination. At present, 7.0T MR examination is not yet allowed for diagnostic use. Therefore, the results of 7.0T MR studies had no influence on oncological therapies of all study participants. All MR examinations were supervised by an experienced radiologist capable of treating allergic reactions, seizures, and other emergencies. The medical staff at the 7.0T site avoided fast table movements in the ultrahigh magnetic field in order to prevent vertigo.
Over a period of 12 months, four consecutive patients with brain metastases (3 women and 1 man) were included in the study. The mean age of the patients was 53.5 years (age range, 46-58 years). The primary cancer types were three lung cancers (2 adenocarcinomas, 1 small cell) and one malignant melanoma.
MR Imaging Techniques
Ultrahigh field MR examinations were performed on a 7.0T whole-body MR system (Magnetom 7.0T, Siemens Healthcare, Erlangen, Germany). The 7.0T magnet, with a clear bore of 90 cm, is equipped with a water cooled gradient and RF coils. The gradient system operates at 2000 V/650 Amp with gradient amplitude of 40 mT/m, a maximum slew rate of 200 mT/m/ms, and a minimum gradient rise time of 200 microseconds. A birdcage TX/RX single channel coil was used. The 1.5T system was a Signa Excite whole-body scanner (GE Healthcare, Milwaukee, WI, USA) with a birdcage head coil.
The time elapsed between the 1.5T and 7.0T MR examinations of each patient ranged from 1 to 10 days (mean interval, 4.5 days). A contrast-enhanced 3D T1-weighted gradient echo sequence with magnetization preparation (3D T1-GRE; MP-RAGE at 7.0T and FSPGR at 1.5T) at 1.5T was compared to a 7.0T MR sequence. For coronal T1-weighted 3D GRE at 7.0T, the acquisition parameters were: TR, 3200-4000 ms; TE, 3.4-44 ms; TI, 1000 ms; FA, 100; section thickness, 0.7-0.8 mm; matrix, 256-448 x 256-448; NEX, 1; and acquisition time, 13 min 29 sec. For axial T1-weighted 3D T1-GRE at 1.5T, the acquisition parameters were: TR, 8.6-11.9 ms; TE, 3.6-5.3 ms; FA, 200; section thickness, 1.5 mm; matrix, 256 x 256; NEX, 2; and acquisition time, 7 min 26 sec.
At 7.0T gadolinium-enhanced 3D T1-GRE images were obtained after injection of a single dose (SD) (0.1 mmol/kg body weight) of gadopentetate dimeglumine (Gd-DTPA) (Magnevist®, Bayer Healthcare Pharmaceuticals Inc., Liverkusen, Germany) in all patients with a 5 minutes delay. The 1.5T 3D T1-GRE sequence was performed with an initial double dose (DD) (0.2 mmol/kg body weight) of Gd-DTPA mine after a 5 minutes delay. For comparison with 1.5T, we generated axial-reformatted T1-GRE images with 1.5 mm slice thickness at 7.0T.
Imaging Analysis
Image analysis was performed by two radiologists in consensus. The number of contrast-enhancing metastases on axial T1-GRE images was counted at both field strengths. In four patients the number of brain metastases on 3D T1-GRE images was compared after administration of SD Gd-DTPA at 7.0T with DD Gd-DTPA administration at 1.5T with a delay of 5 minutes.
Quantitative image assessment was performed subsequently. Signal intensities of individual types of tissue and lesions were assessed by region of interest (ROI) measurements with ROI values placed identically on both series of images using the same sized circular ROI from the software available on both scanners. Lesion-to-brain-contrast for the lesion was evaluated as follows.
Numerical tumor-to-brain-contrast after gadolinium administration (TB contrast ratio) is defined as:
TB contrast ratio = (TB - NW)/NW
With TB taken as the signal intensity of an ROI assessed over a lesion after contrast agent administration and NW taken as the signal intensities assessed over the normal appearing deep white matter. The signal intensity of a lesion was measured within an enhanced area. In inhomogeneously enhanced tumors, the area of maximum uptake was chosen for measurement.
Statistical Analysis
The signal intensity values in the quantitative measurements were expressed as mean ± standard deviation. The paired t test was used to compare the tumor-to-brain contrast ratio between 7.0T and 1.5T. For all tests, significance was set at P < 0.05, and SPSS software package (SPSS 16.0, Chicago, IL, USA) was used for statistical analyses.
RESULTS
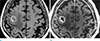
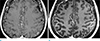
No allergic reactions were observed after intravenous application of Gd-DTPA at both field strengths. Among four patients, a total of 11 brain metastases were detected by two radiologists at the 1.5T 3D T1-GRE sequence after DD of Gd-DTPA and 7.0T 3D T1-GRE sequence after SD of Gd-DTPA (Fig. 1).
In the quantitative analysis of contrast ratios of enhancing brain metastases and white matter, the 1.5T 3D T1-GRE after DD showed an increased TB contrast ratio compared to 7.0T 3D T1-GRE after SD (0.961 ± 0.571 versus 0.885 ± 0.494; n = 11 metastases). But this difference was not statistically significant (P = 0.711) (Fig. 2).
DISCUSSION
Limiting the easy clinical implementation of ultra-high field MRI (≥ 7.0T) is the fact that human dimensions are no longer a negligible fraction of the wavelength of radiofrequency radiation, leading to radiofrequency field (B1) inhomogeneity that compromises image quality. In addition, magnetic field (B0) inhomogeneities produced by air/water interfaces or mineralization become amplified at 7.0T compared to lower field strengths. Higher energy absorption (measured by the specific absorption ratio, or SAR) constrains sequence development. Nevertheless, the most dominant benefit of high magnetic field strengths in MR imaging is the approximately linear enhancement of image signal-to-noise ratio (SNR).
Ultra-high field 7.0T MRI offers superior SNR relative to any other noninvasive imaging technique. The higher signal-to-noise ratio can be used to increase scan speed and/or to obtain a higher resolution (18, 19) and where the higher spectral resolution (20) and the increased sensitivity for various contrast mechanisms such as blood oxygenation level-dependent (BOLD) (21) have proven useful. The increased SNR leads to a higher contrast-to-noise ratio (CNR) between enhancing and non-enhancing tissues. In addition, with the longer baseline relaxation times brought about by the higher magnetic field strength, the T1-shortening effect of Gd-based contrast agents should be greater and the contrast enhancement of the lesions on T1-weighted images should generally be stronger at 3.0T than they are at 1.5T (22). The significantly enhanced sensitivity at 7.0T may prove to be a decisive advantage for the diagnosis of tumorous entities (23). In a preliminary study, the detection of metastases of bronchial carcinomas in single-dose gadolinium contrast-enhanced MRI at 7.0T was almost equivalent to the sensitivity at double-dose 1.5T (198 versus 238 brain metastases) (24). Our results are similar to this study.
The standard dose of contrast for 1.5T MR imaging systems is 0.1 mmol/kg body weight. It has been shown that greater sensitivity can be achieved when higher doses, up to 0.3 mmol/kg gadolinium are administered (8, 9, 10). In a larger series specifically evaluating brain metastasis, it was shown that triple-dose gadolinium MRI increases mean lesion contrast, increases qualitative conspicuity of lesions, detects additional small lesions and, in a subset of patients, would have changed choice of therapy (25). Lesions greater than 10 mm will be seen at all dose levels. The utility of higher dose gadolinium mainly lies in the ability to reveal smaller lesions, especially less than 5 mm (25, 26). However, the use of a higher dose of contrast medium not only increases the potential side effects, but also represents a substantial increase in cost, compared to a standard 0.1 mmol/kg dose. Since early 2006 evidence has accumulated that some gadolinium based contrast agents, particularly gadodiamide (Omniscan, GE Healthcare, Chalfont St. Giles, UK), may cause a potentially devastating or even fatal scleroderma-like, fibrosing condition called nephrogenic systemic fibrosis (NSF) in patients with renal failure (27, 28, 29). Recently, it has been shown that gadopentetate dimeglumine (Magnevist, Bayer Schering, Berlin, Germany) may also trigger NSF, but apparently not with the same high frequency as gadodiamide. Therefore, we concern to use high dose gadolinium based contrast agents.
There are two limitations in this study. First limitation of this study is that the number of patients in our study was too small, making the sensitivity data less robust than the specificity data. Second limitation is different spatial resolution in each contrast-enhanced MRI protocol.
In conclusion, we suggest that assessment of possible brain metastases using 0.1 mmol/kg Gd-DTPA with a 7.0T MR imaging system is comparable to 0.2 mmol/kg Gd-DTPA at 1.5T.
 XML Download
XML Download