

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The heart consists of three major segments, namely, the atria together with the systemic and pulmonary veins, the ventricles with their atrioventricular valves and the great arteries with their outflow tracts (1). Anatomy of the malformed heart can be evaluated, classified and presented by segmental approach, which utilizes a simple notation system that enables rapid communication (2). The notation system consists of a group of three letters/parts, which gives respective information on the three major cardiac segments in terms of the visceroatrial situs, the orientation of the ventricular loop, and the relation of the great vessels (23). Supplementary information on the atrioventricular and ventriculoarterial connections and associated anomalies should be added to the three-part notation system for clear, precise description. The following paragraphs summarize the steps of Van Praagh's segmental approach.
Step One - Visceroatrial Situs
Firstly, visceral situs is determined by the broncho-pulmonary anatomy and location of the liver, stomach and spleen (3). Morphological right lung has three lobes and its main bronchus in an eparterial position, i.e. directly behind the pulmonary artery (Fig. 1a). The morphological left lung has two lobes with its main bronchus in a hyparterial position, i.e. inferior to the pulmonary artery (23) (Fig. 1b).
Next, atrial situs is determined. Anatomical features such as crista terminalis and broad appendage of the morphological right atrium can help distinguish it from the left atrium which has narrow tubular appendage. But these features may not always be easy to identify on imaging. The rule of venoatrial concordance would be helpful to determine the atrial situs (23), the morphological right atrium usually receives systemic venous return.
Situs solitus (S, _, _) is defined as morphological right lung, morphological right atrium and largest lobe of liver on patient's right side; morphological left lung, morphological left atrium, spleen and stomach on patient's left side. Situs inversus (I, _, _) is designated when all the anatomical structures are inversed. If the patient's anatomy does not fit either solitus or inversus, situs ambiguous (A, _, _) is designated (2).
Step two - Orientation of Ventricular Loop
The following table shows some helpful features to distinguish morphological right and left ventricles (2).
(_,D,_) is designated when the morpholoigcal right ventricle is located on the right side of morphological left ventricle, i.e. D-loop. (_,L,_) is designated if their sides are reversed.
Step three - Position and Relation of the Great Vessels
The great vessels relation is analyzed at the level of the aortic and pulmonary valves, if these structures are difficult to identify on imaging, the aortic root and main pulmonary trunk are identified for analysis.
The normal solitus position (_,_, S) is defined as aorta right posterior to the main pulmonary artery (23) (Fig. 1c) The mirror image of this relation with aorta left posterior to the main pulmonary artery is designated as inversus (_,_,I) (23). Transposition is usually seen with the aorta anterior to the main pulmonary artery, with right anterior being dextrotransposition (_,_,D-TGV) (Fig. 2a); and levotransposition (_,_,L-TGV) when aorta is left anterior to main pulmonary artery (23) (Fig. 2b) A side-by-side relation of aorta and main pulmonary artery in the coronal plane is usually described as malposition, with D-malposition (_,_,D-MGV) and L-malposition (_,_,L-MGV) if the aorta is rightward of and leftward of main pulmonary artery respectively (2).
Finally, to complete the picture, further details on atrioventricular connection, ventriculoarterial connection, and associated abnormalities would give accurate anatomical diagnosis (3). Atrioventricular connection may be concordant, discordant or ambiguous when there are two ventricles (3). In case of univentricular heart, the atrioventricular connection may be double inlet and absent right/left connection (3). Ventriculoarterial connection may be described as concordant, discordant or double outlet right / left ventricle (3).
Case 1
A newborn baby girl developed chest retraction after birth. Findings of atrioventricular septal defects were detected on echocardiogram. The patient's visceral, cardiac and vascular anatomy was well demonstrated by cardiac MRI and CT.
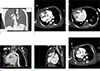
Step one (Fig. 3a-c)
Patient's visceroatrial situs is shown to be situs ambiguous with left isomerism.
Case 2
An eight years old girl with antenatal diagnosis of congenitally corrected transposition of great vessels. She remains well with satisfactory exercise tolerance. She is planned for observational management. The patient's anatomy is well demonstrated by MRI.
Case 3
A three years old boy with antenatal diagnosis of atrioventricular septal defect. He was born at 37 weeks by normal delivery. He had severe atrioventricular valve regurgitation and was treated by pulmonary arterial banding and valvular repair at one month old, bidirectional cavopulmonary shunt was performed at six-month old. The patient's anatomy is demonstrated by pre-operative CT.
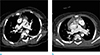
Step one (Fig. 5a-b)
Patient's visceroatrial situs is shown to be situs ambiguous with right isomerism.
CONCLUSION
Cardiovascular anatomy is analyzed in a stepwise fashion based on segmental situs and alignments (4). Segmental approach can give a concise anatomical diagnosis for congenital heart disease. Its simplicity allows effective communication among specialists. Complicated cases can also be accurately characterized.




 XML Download
XML Download