

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Acute disseminated encephalomyelitis (ADEM) is a demyelinating and inflammatory condition of the central nervous system (CNS) and usually presents with multifocal neurological deficits and altered mental status (1). It occurs after systemic viral infections or vaccinations. ADEM also usually affects the white matter in the brain and spinal cord.
Imaging studies, such as brain CT or MRI are needed to make the diagnosis of ADEM, by detection of the typical anatomical lesions in combination with the patient's clinical history. However, patients with an unusual lesion location, not involving white matter, may be difficult to diagnose and experience delays in their treatment. As far as we know, only a few cases of ADEM in patients with a single brainstem lesion have been reported in the literature. Here, we report a very rare case of a girl showing isolated involvement of the rhombencephalon in ADEM, mimicking viral rhombencephalitis on brain CT and MR images.
CASE REPORT
A 4-year-old Asian girl living in South Korea developed a painful sensation extending from her right thigh to ankle 5 days prior to admission. Two days later, she started to complain of general weakness, headache, gait disturbance, ataxia, dysarthria, dyspnea, and acalculia.
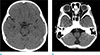
After admission, CSF and blood analyses, and imaging studies (CT and MRI) were performed. Her protein level in CSF was high (291.3 mg/dL), but other values such as white blood cell counts and viral markers were within normal limits. On CT scans, suspicious ill-defined low-density lesions in the pons and medulla were seen (Fig. 1). After 2 days, brain MRI was performed. On the MR scan, T2 high signal intensity (T2-HSI) lesions with mild swelling were present in the pons, both middle cerebellar peduncles, and the anterior medulla. Diffusion-weighted imaging showed no diffusion restriction at the sites of the T2-HSI lesions, suggesting vasogenic rather than cytotoxic edema. There was no definite lesion enhancement on the MR image (Fig. 2).
Administration of IV globulin, antiviral agents, and steroids was started because viral rhombencephalitis and other demyelinating diseases such as ADEM or vasculitis cannot be differentiated. However, after careful history taking, a history of upper respiratory infection (1 month earlier) and enterocolitis (2 weeks earlier) was discovered. In addition, she had experienced fever 10 days ago, for 3 days, because of acute otitis media. Thus, her anti-viral agents were discontinued and she was maintained on steroids; her symptoms were gradually relived.
After 18 days of admission, a follow-up brain MRI was performed, which showed a decreased extent of the T2-HSI lesions in the pons, medulla, and both middle cerebellar peduncles. Additionally, its margin was more prominent (Fig. 3).
Her symptoms were completely relieved after 3 weeks, and she was discharged.
DISCUSSION
ADEM is a demyelinating and inflammatory condition of the CNS and usually presents with multifocal neurological deficits and altered mental status (1). It is usually regarded as a monophasic disease. Recurrent ADEM involves the same anatomical area as the initial illness involved, and recurs up to 3 months of the initial event (12). If these relapses involve different anatomical areas in MRI, or new focal neurological deficits occur, it indicates multiphasic ADEM (3).
ADEM usually occurs after systemic viral infections or vaccinations, and often follows common childhood infections such as measles, mumps, rubella, and chickenpox, or vaccination to these microorganisms (4).
ADEM can occur at any age, but is most common in prepubescent. Peak incidence is between 3 and 10 years, because of the frequency of immunizations and antigen exposure. ADEM has no clear sex predominance (124).
Within 1-2 weeks of a systemic infection or vaccination, ADEM presents with acute symptoms, including fever, headache, convulsions, encephalopathy, and multifocal neurological deficits (56). ADEM most frequently involves multifocal white matter and also involves deep gray matter, the corona radiata, and the centrum semiovale. However, it does not usually involve the calloseptal interface (67).
ADEM has overlapping symptoms and imaging findings with a broad spectrum of CNS diseases, which can cause misdiagnoses. Commonly, ADEM needs to be differentiated from several diseases, including brain stem glioma, multiple sclerosis, infectious encephalitis, CNS involvement of connective tissue disorders, and other types of vasculitis (systemic lupus erythematosus, Neuro-Behcet disease, and neurosarcoidosis). When the lesion involves the brain stem, other brain stem lesions such as infectious brain stem encephalitis, rhombencephalitis, abscesses, tuberculomas, toxoplasmosis, histoplasmosis, metastasis, and diffuse mesencephalic gliomas could also be considered (68).
ADEM has variable clinical symptoms and no specific biological markers; the diagnosis of ADEM is considerably dependent on clinical history and sequential MR imaging. If the diagnosis of ADEM is not certain, serial follow-up MR imaging is needed, so as to exclude several likely differential diagnoses. ADEM is generally regarded as a monophasic disease, and does not typically exhibit a new lesion on the follow-up exam (689).
Our case had unusual multifocal lesions confined to the rhombencephalon. Only a few similar cases have been reported in previous articles (6810). In the reported cases, T2-HSI lesions with mild swelling were present in only the rhombencephalon, including the pons, both middle cerebellar peduncles, and the anterior medulla (68). In the study by Alper et al. (8), 3 of 112 pediatric patients with acute demyelinating syndromes showed isolated brain stem involvement. After an extensive work-up and MRI follow-up, these three cases of acute demyelinating syndromes was concluded as a localized form of ADEM with a favorable prognosis. At first, we thought that our patient was affected by viral rhombencephalitis because the areas of involvement, in the brain stem without involvement of white matter or deep gray matter, were very unusual in ADEM. However, after reinvestigation with careful history taking, it was found that she had a prior history of upper respiratory infection (1 month earlier) and enterocolitis (2 weeks earlier). Neuroimaging findings and multifocal neurological symptoms including headache, gait disturbance, ataxia, dysarthria, and acalculia, with no evidence of acute CNS infection such as negative viral markers in CSF, were suggestive of ADEM mimicking viral rhombencephalitis. Additionally, no microorganisms were cultured in the patient's CSF. So, it was regarded as an unusual case of ADEM rather than viral encephalitis. Combined antiviral and steroid pulse therapy was performed.
MRI is effective in monitoring the disease process (6). On follow-up brain MRI performed 18 days after onset, the T2-HSI lesions had partially improved in the pons, both middle cerebellar peduncles, and the medulla.
In ADEM, patient history, CSF and blood analyses, and neuroimaging findings are essential for diagnosis. However, it should be kept in mind that ADEM can involve unusual sites such as the rhombencephalon in isolation, without involvement of the white matter or deep gray matter. Thus, ADEM should be considered even when it appears in unusual anatomical areas, and detailed history taking must be performed and clinical information should be obtained.


 XML Download
XML Download