

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
We analyzed the outcome of medical management for children with vesicoureteral reflux (VUR) and we determined the factors affecting the outcome.
Materials and Methods
We retrospectively reviewed the records of 37 patients (56 kidneys) who were diagnosed with VUR between 1995 and 2004. All the patients were maintained on prophylactic antibiotics and had regular follow up. The subjects were stratified according to the grade of reflux at the time of diagnosis into the low grade group (grade III or below) or the high grade group (grade IV or above), based upon the International Classification System. The effects of the reflux grade, the presence or absence of renal scar, the age at diagnosis, laterality of disease and gender on the improvement/resolution rate of VUR were analyzed.
Results
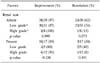
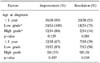
The mean duration until resolution was 35 months. Improvement occurred in 48 kidneys, including resolution in 27 kidneys. The resolution rate was higher in the kidneys with low grade reflux than that in the kidneys with high grade reflux. The resolution rate was higher in kidneys without scar than that in the kidneys with scar. A significantly higher improvement rate was observed for the children diagnosed before 1 year of age than that for the children diagnosed after 1 year of age.
Figures and Tables

Table 2
Medical treatment outcome of vesicoureteral reflux (VUR) according to gender, age at diagnosis, the reflux grade, presence or absence of renal scar and laterality of disease

References
1. Elder JS. Guidelines for consideration for surgical repair of vesicoureteral reflux. Curr Opin Urol. 2000. 10:579–585.
2. Lebowitz RL, Olbing H, Parkkulainen KV, Smellie JM, Tamminen-Möbius TE. International system of radiographic grading of vesicoureteric reflux. International Reflux Study in Children. Pediatr Radiol. 1985. 15:105–109.
3. Arant BS Jr. Medical management of mild and moderate vesicoureteral reflux: followup studies of infants and young children. A preliminary report of the Southwest Pediatric Nephrology Study Group. J Urol. 1992. 148:1683–1687.
4. Levit SB, Duckett J, Spitzer A, Walker D, Weiss R, Lebowitz R, et al. Medical versus surgical treatment of primary vesicoureteral reflux: a prospective international reflux study in children. J Urol. 1981. 125:277–283.
5. Wheeler D, Vimalachandra D, Hodson EM, Roy LP, Smith G, Craig JC. Antibiotics and surgery for vesicoureteric reflux: a meta-analysis of randomized controlled trials. Arch Dis Child. 2003. 88:688–694.
6. Heidenreich A, Ozgur E, Becker T, Haupt G. Surgical management of vesicoureteral reflux in pediatric patients. World J Urol. 2004. 22:96–106.
7. Smellie JM, Jodal U, Lax H, Möbius TT, Hirche H, Olbing H. Outcome at 10 years of severe vesicoureteric reflux managed medically: report of the International Reflux Study in Children. J Pediatr. 2001. 139:656–663.
8. Atala A, Keating MA. Walsh PC, Retik AB, Vaughan ED, Wein AJ, editors. Vesicoureteral reflux and megaureter. Campbell's urology. 2002. 8th ed. Philadelphia: Saunders;2053–2116.
9. Arant BS Jr. Vesicoureteral reflux and evidence-based management. J Pediatr. 2001. 139:620–621.
10. Riedmiller H, Androulakakis P, Beurton D, Kocvara R, Gerharz E. European Association of Urology. EAU guidelines on paediatric urology. Eur Urol. 2001. 40:589–599.
11. Hong DH, Sohn JW, Lee CH, Kim JI. Treatment of primary vesicoureteral reflux in children. Korean J Urol. 1993. 34:97–102.
12. Ransley PG. Vesicoureteric reflux: continuing surgical dilemma. Urology. 1978. 12:246–255.
13. McLorie GA, McKenna PH, Jumper BM, Churchill BM, Gilmour RF, Khoury AE. High grade vesicoureteral reflux: analysis of observational therapy. J Urol. 1990. 144:537–540.
14. Lenaghan D, Whitaker JG, Jensen F, Stephens FD. The natural history of reflux and long-term effects of reflux on the kidney. J Urol. 1976. 115:728–730.
15. Cavanagh PM, Sherwood T. Too many cystograms in the investigation of urinary tract infection in children? Br J Urol. 1983. 55:217–219.
16. Kim SY, Shin KY, Woo YN. Renal scarring in surgically treated primary vesicoureteral reflux. Korean J Urol. 2001. 42:894–899.
17. Rolleston GL, Maling TM, Hodson CJ. Intrarenal reflux and the scarred kidney. Arch Dis Child. 1974. 49:531–539.
18. Rose JS, Glassberg KI, Waterhouse K. Intrarenal reflux and its relationship to renal scarring. J Urol. 1975. 113:400–403.
19. Lama G, Tedesco MA, Graziano L, Calabrese E, Grassia C, Natale F, et al. Reflux nephropathy and hypertension: correlation with the progression of renal damage. Pediatr Nephrol. 2003. 18:241–245.
20. Hwa JS, Chung KH. Renal scar in vesicoureteral reflux. Korean J Urol. 1996. 37:538–542.
21. Yeung CK, Godley ML, Dhillon HK, Gordon I, Duffy PG, Ransley PG. The characteristics of primary vesico-ureteric reflux in male and female infants with pre-natal hydronephrosis. Br J Urol. 1997. 80:319–327.
22. Aladjem M, Boichis H, Hertz M, Herzfeld S, Raviv U. The conservative management of vesicoureteric reflux: a review of 121 children. Pediatrics. 1980. 65:78–80.
23. Tamminen-Möbius T, Brunier E, Ebel KD, Lebowitz R, Olbing H, Seppanen U, et al. Cessation of vesicoureteral reflux for 5 years in infants and children allocated to medical treatment. The International Reflux Study in Children. J Urol. 1992. 148:1662–1666.
24. Sjöstrom S, Sillen U, Bachelard M, Hansson S, Stokland E. Spontaneous resolution of high grade infantile vesicoureteral reflux. J Urol. 2004. 172:694–698.
25. Chand DH, Rhoades T, Poe SA, Kraus S, Strife CF. Incidence and severity of vesicoureteral reflux in children related to age, gender, race and diagnosis. J Urol. 2003. 170:1548–1550.
26. Schwab CW Jr, Wu HY, Selman H, Smith GH, Snyder HM 3rd, Canning DA. Spontaneous resolution of vesicoureteral reflux: a 15-year perspective. J Urol. 2002. 168:2594–2599.
27. Choi SK. Reflux nephropathy in children. Korean J Urol. 1983. 24:873–877.
 XML Download
XML Download