

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
One of the most serious complications of benign prostatic hyperplasia (BPH) is acute urinary retention (AUR). Up to now, many papers have evaluated the short term treatment of patients with AUR that is due to BPH. Therefore, we evaluated the long term follow-up of BPH patients with AUR.
Materials and Methods
154 BPH patients with AUR were divided into two groups. One group was considered to be the failure cases of urethral catheter removal, and this group (55 patients) had undergone immediately transurethral resection of prostate (TURP). The other group was considered to be the successful cases of urethral catheter removal. The latter group was divided into 3 groups: the α-blocker group, the α-blocker with 5 α-reductase inhibitor group and the suprapubic cystostomy with medical treatment group. We evaluated the long term follow-up of these groups and the changes of treatment for 1 month, 3 months, 6 months and 12 months.
Results
The mean volume of the prostate was 54.2ml. When the patients were admitted to the hospital due to AUR, 53% of the patients had previously experienced AUR, and the mean number of previous AUR episodes were 1.4 times. The initial management of AUR due to BPH was urethral catheter indwelling with medical treatment. If the catheter removal failed, TURP was perfomed (35%) and when successful, medical treatment was then done.
Conclusions
The primary management of AUR due to BPH is urethral catheter indwelling with medical treatment (α-blocker). However, if the patients have a large size prostate, we should first consider hormone treatment (5 α-reductase inhibitor) rather than surgical treatment. The management methods of some patients were changed during the follow-up. Therefore, when following up these cases, we should be careful to prevent the recurrence of AUR and to allow self-voiding.
Figures and Tables
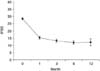 | Fig. 1The change of the IPSS for the medical treatment patients. IPSS: International Prostate Symptom Score.
|



References
1. Girman CJ, Epstein RS, Jacobsen SJ, Guess HA, Panser LA, Oesterling JE, et al. Natural history of prostatism: impact of urinary symptoms on quality of life in 2115 randomly selected community men. Urology. 1994. 44:825–831.
2. Birkhoff JD, Wiederhorn AR, Hamilton ML, Zinsser HH. Natural history of benign prostatic hypertrophy and acute urinary retention. Urology. 1976. 7:48–52.
3. Abrams P. Objective evaluation of bladder oulet obstruction. Br J Urol. 1995. 76:Suppl 1. 11–15.
4. Jacobson SJ, Jacobson DJ, Girman CJ, Roberts RO, Rhodes T, Guess HA, et al. Natural history of prostatism: risk factors for acute urinary retention. J Urol. 1997. 158:481–487.
5. Guess HA. Benign prostatic hyperplasia: antecedents and natural history. Epidemiol Rev. 1992. 14:131–153.
6. Barry MJ, Fowler FJ, Bin L, Pitts JC III, Harris CJ, Mulley AG Jr. The natural history of patients with benign prostatic hyperplasia as diagnosed by North American urologists. J Urol. 1997. 157:10–14.
7. Kurita Y, Masuda H, Terada H, Suzuki K, Fujita K. Transitional zone index as a risk factor for acute urinary retention in benign prostatic hyperplasia. Urology. 1998. 51:595–600.
8. Powell PH, Smith PJ, Feneley RC. The identification of patients at risk from acute retention. Br J Urol. 1980. 52:520–522.
9. O'Flynn JD. The management of simple prostatic hyperplasia. Br J Hosp Med. 1969. 2:562.
10. Breum L, Klarskov P, Munck LK, Nielsen TH, Nordestgaard AG. Significance of acute urinary retention due to intravesical obstruction. Scand J Urol Nephrol. 1982. 16:21–24.
11. Mebust WK, Holtgrewe HL, Cockett AT, Peters PL. Transurethral prostatectomy: immediate and postoperative complications. A cooperative study of 13 participating institutions evaluating 3,885 patients. J Urol. 1989. 141:243–247.
12. Pickard R, Emberton M, Neal DE. The management of men with acute urinary retention. Br J Urol. 1998. 81:712–720.
13. Schulman CC. Long-term aspects of medical treatment of BPH. Eur Urol. 2001. 40:Suppl 3. 8–12.
14. McConnell JD, Roehrborn CG, Bautista OM, Andriole GL Jr, Dixon CM, Kusek JW, et al. The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of benign prostatic hyperplasia. N Engl J Med. 2003. 349:2387–2398.
15. Roehrborn CG, Bruskewitz R, Nickel GC, Glickman S, Cox C, Anderson R, et al. Urinary retention in patients with BPH treated with finasteride or placebo over 4 years. Characterization of patients and ultimate outcomes. Eur Urol. 2000. 37:528–536.
16. Fontanarosa PB, Roush WR. Acute urinary retention. Emerg Med Clin North Am. 1988. 6:419–437.
17. Caine M, Perlberg S. Dynamics of acute urinary retention in prostatic patient and role of adrenergic receptors. Urology. 1977. 9:399–403.
18. Choong S, Emberton M. Acute urinary retention. BJU Int. 2000. 85:186–201.
19. Manikandan R, Srirangam SJ, O'Reilly PH, Collins GN. Management of acute urinary retention secondary to benign prostatic hyperplasia in the UK: a national survey. BJU Int. 2004. 93:84–88.
20. Cho DK, Chang SG. The clinical study of acute urinary retention in patients with benign prostate hyperplasia. Korean J Urol. 2000. 41:212–217.
21. McNeill SA, Hargreave TB. Alfuzosin once daily facilitates return to voiding in patients in acute urinary retention. J Urol. 2004. 171:2316–2320.
22. McNeill SA, Hargreave TB, Roehrborn CG. Alfuzosin 10 mg once daily in the management of acute urinary retention: results of a double-blind placebo-controlled study. Urology. 2005. 65:83–89.
23. Lucas MG, Stephenson TP, Nargund V. Tamsulosin in the management of patients in acute urinary retention from benign prostatic hyperplasia. BJU Int. 2005. 95:354–357.
24. McNeill SA, Daruwala PD, Mitchell ID, Shearer MG, Hargreave TB. Sustained-release alfuzosin and trial without catheter after acuter urinary retention: a prospective, placebo-controlled. BJU Int. 1999. 84:622–627.
25. Gormley GJ, Stoner C, Bruskewitz RC, Imperato-McGinley J, Walsh PC, McConnell JD, et al. The effect of finasteride in men with benign prostatic hyperplasia. N Engl J Med. 1992. 327:1185–1191.
26. Kaplan SA, Reis RB, Cologna A, Suad HJ, Martins AC, Kohn IJ, et al. Intermittent alpha-blocker therapy in the treatment of men with lower urinary tract symptoms. Urology. 1998. 52:12–16.
27. Muldowney FP, Duffy GJ, Kelly DG, Duff FA, Harrington C, Freaney R. Sodium diuresis after relief of obstructive uropathy. N Engl J Med. 1966. 274:1294–1298.
 XML Download
XML Download