

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Mixed connective tissue disease (MCTD) was first described by Sharp and coworkers in 1972, characterized by symptoms of Raynaud's phenomenon or swollen hands, overlapping clinical features of systemic lupus erythematosus, systemic sclerosis, or polymyositis/dermatomyositis, and the presence of anti-U1 RNP antibody. MCTD is rare in children and constitutes 0.3~0.6% of all rheumatologic patients in pediatric rheumatology database of the United States. Here, we report the first Korean case of a 10-year-old female patient with MCTD, presenting Raynaud's phenomenon in the hands, feet, and tongue.
Figures and Tables
 | Figure 1Raynaud's phenomenon in the fingertips. Demarcated digital pallor and cyanosis developed after exposure to cold.
|

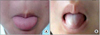 | Figure 3Raynaud's phenomenon in the tongue. The photographs show color changes from red (A) to pallor and (B) after cold application.
|
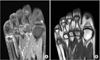 | Figure 4Magnetic Resonance Imaging (MRI) images of the right Foot. MRI shows focal low T1 signal intensity (A) and high T2 signal intensity (B) at the head of the second and fifth metatarsal bone, consistent with bone marrow edema. Scanty effusion is seen at the second and fifth metatarsophalangeal joint.
|
References
1. Sharp GC, Irvin WS, Tan EM, Gould RG, Holman HR. Mixed connective tissue disease--an apparently distinct rheumatic disease syndrome associated with a specific antibody to an extractable nuclear antigen (ENA). Am J Med. 1972. 52:148–159.
2. Block JA, Sequeira W. Raynaud's phenomenon. Lancet. 2001. 357:2042–2048.
3. Alarcon-Segovia D, Villareal M. Kasukawa R, Sharp GC, editors. Classification and diagnostic criteria for mixed connective tissue disease. Mixed connective tissue disease and anti-nuclear antibodies. 1987. Amsterdam: Excerpta Medica;33–40.
4. Kasukawa R, Tojo T, Miyawaki S. Kasukawa R, Sharp GC. Preliminary diagnostic criteria for classification of mixed connective tissue disease. Mixed connective tissue disease and anti-nuclear antibodies. 1987. Amsterdam: Excerpta Medica;41–48.
5. Grader-Beck T, Wigley FM. Raynaud's phenomenon in mixed connective tissue disease. Rheum Dis Clin North Am. 2005. 31:465–481. vi
6. Mier RJ, Shishov M, Higgins GC, Rennebohm RM, Wortmann DW, Jerath R, et al. Pediatric-onset mixed connective tissue disease. Rheum Dis Clin North Am. 2005. 31:483–496.
7. Bridges MJ, Kelly CA. Raynaud's phenomenon affecting the tongue of a patient with scleroderma. Ann Rheum Dis. 2002. 61:472.
8. Rosato E, Salsano F. Raynaud phenomenon of the tongue in a patient with scleroderma. J Clin Rheumatol. 2010. 16:201.
9. Tiddens HA, van der Net JJ, de Graeff-Meeder ER, Fiselier TJ, de Rooij DJ, van Luijk WH, et al. Juvenile-onset mixed connective tissue disease: longitudinal follow-up. J Pediatr. 1993. 122:191–197.
 XML Download
XML Download