 PDF
PDF ePub
ePub Citation
Citation Print
Print


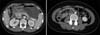
The patient, an 18-year-old woman, presented with upper abdominal pain. She was diagnosed systemic lupus erythematosus (SLE) 3 years ago. Figure 1 was abdominal computed tomography (CT) at that time. CT showed gastric wall edema and thickening. However, small intestine and large bowel were intact. Gastroscopy showed mucosal edema and erythema from lesser curvature to antrum (Figure 2). Gastric mucosal biopsy was just chronic gastritis. She was diagnosed lupus mesenteric vasculitis (LMV) limited in gastric wall. We ordered intravenous steroid therapy (1 mg/kg/day), and abdominal pain was improved. LMV is life-threatening unless proper management and more frequent in patient of SLEDAI >5. Most of LMV patients showed abdominal plain film characteristic of paralytic ileum. But, enhanced abdominal CT is most powerful diagnostic tool (1). Therefore, CT is valuable diagnostic tool in SLE patients with severe abdominal pain without evidence of paralytic ileus in abdominal plain film.
- About Synapse
- How to Participate
- KAMJE Databases


- About Synapse
- How to Participate
- KAMJE Databases
Journal List > J Rheum Dis > v.19(4) > 1063981

- TOOLS
 XML Download
XML Download- Similar articles