

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background
Prader-Willi syndrome (PWS) is a congenital disorder, which is clinically characterized by a short stature, muscular hypotonia, hypogonadism, mental retardation and hyperphagia, leading to early childhood obesity. Impaired growth hormone (GH) secretion, hypogonadism, and obesity are common in patients with PWS. The purpose of this study was to find the effects of growth hormone treatment in patients with PWS.
Methods
Six patients with PWS confirmed by a genetic study were recruited, and treated with growth hormone (Eutropin®) (0.8-1 IU/kg/week) divided into five or seven day doses per week for six months. The heights and weights of the subjects were evaluated. GH status were evaluated using the serum insulin-like growth factor (IGF)-I level, the L-dopa test, and insulin-induced hypoglycemia tess. Glucose metabolism was evaluated using the random serum glucose and HbA1c levels.
Results
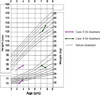
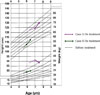
GH was found to be deficient in 2 out of 6 subjects by the insulin test, in 3 out of 6 by the IGF-I level, and in 5 out of in 5 by the L-dopa test. After six months of GH treatment, the height percentile was increased and weight percentile decreased. The serum glucose and HbA1c levels remained unchanged.
Figures and Tables








References
1. Prader A, Labhart A, Willi H. Ein syndrome von dipostas, kleinwuchs, kryptorchismus, und oligophrenie nach myotonieartigen zustand im neugeborenalter. Schwei Med Whchr. 1956. 86:1260–1261.
2. Zellweger H, Schneider HJ. Syndrome of hypotonia-hypopigmentia-hypogonadism-obesity (HHHO) or Prader-Willi syndrome. Am J Dis Child. 1968. 115:588–598.
5. Angulo M, Castro-Magana M, Mazur B, Canas JA, Vitollo PM, Sarrantonio M. Growth hormone secretion and effects of growth hormone therapy on growth velocity and weight gain in children with Prader-Willi syndrome. J Pediatr Endocrinol Metab. 1996. 9:393–400.
6. Thacker MJ, Hainline B, Dennis-Feezle L, Johnson NB, Pescovitz OH. Growth failure in Prader-Willi syndrome is secondary to growth hormone deficiency. Horm Res. 1998. 49:216–220.
7. Hauffa BP. One-year results of growth hormone treatment of short stature in Prader-Willi syndrome. Acta Paediatr Suppl. 1997. 423:63–65.
8. Lindgren AC, Hagenas L, Muller J, Blichfeldt S, Rosenborg M, Brismar T, Ritzen EM. Effects of growth hormone treatment on growth and body composition in Prader-Willi syndrome: a preliminary report. Acta Paediatr Suppl. 1997. 423:60–62.
9. Eiholzer U, Weber R, Stutz K, Steinert H. Effect of 6months of growth hormone treatment in young children with Prader-Willi syndrome. Acta Paediatr Suppl. 1997. 423:66–68.
10. Davies PA, Evans S, Broomhead S, Clough H, Day JM, Laidlaw A, Barnes ND. Effect of growth hormone on height, weight, and body composition in Prader-Willi syndrome. Arch Dis Child. 1998. 78:474–476.
11. Lindgren AC, Hagenas L, Muller J, Blichfeldt S, Rosenborg M, Brismar T, Ritzen EM. Growth hormone treatment of children with Prader-Willi syndrome affects linear growth and body composition favourably. Acta Paediatr. 1998. 87:28–31.
12. Myers SE, Carrel AL, Whitman BY, Allen DB. Sustained benefit after 2years of growth hormone on body composition, fat utilization, physical strength and agility and growth in Prader-Willi syndrome. J Pediatr. 2000. 137:42–49.
13. Carrel AL, Myers SE, Whitman BY, Allen DB. Growth hormone improves body composition, fat utilization, physical strength and agility, and growth in Prader-Willi syndrome: A controlled study. J Pediatr. 1999. 134:215–221.
15. Lee PDK, Wilson DM, Rountree L. Linear growth response to exogenous growth hormone in Prader-Willi syndrome. Am J Med Genet. 1987. 28:865–871.
16. Carrel AL, Myers SE, Whitman BY, Allen DB. Sustained benefits of growth hormone on body composition, fat utilization, physical strength and agility, and growth in Prader-Willi syndrome are dose-dependent. J Pediatr Endocrinol Metab. 2001. 14:1097–1105.
17. Carrel AL, Allen DB. Prader-Willi syndrome: how does growth hormone affect body composition and physical function? J Pediatr Endocrinol Metab. 2001. 14:Suppl6. 1445–1451.
18. Burman P, Ritzen EM, Lindgren AC. Endocrine dysfunction in Prader-Willi syndrome: a review with special reference to GH. Endocr Rev. 2001. 22:787–789.
19. Carrel AL, Myers SE, Whitman BY, Allen BY. Benefits of long-term GH therapy in Prader-Willi syndrome: a 4 year study. J Clin Endocrinol Metab. 2002. 87:3590–3597.
20. Kazuo O, Satoru S, Atsunori Y, Nobuyuki M, Ryoichi S. Effects of 5 years growth hormone treatment in patients with Prader-Willi syndrome. J Pediatr Endocrinol Metab. 2003. 16:155–162.
 XML Download
XML Download