

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
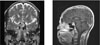
Pituitary tumor can be accompanied with various pituitary hormone abnormalities. Pituitary tumors can be divided into functioning or nonfunctioning tumors. A functioning pituitary tumor, via the oversecretion of pituitary hormones, causes diverse clinical features. A nonfunctioning pituitary tumor can be accompanied with pituitary dysfunction and this may be due to compression or destruction of normal pituitary tissue, suppression of the pituitary portal system or direct damage to the hypothalamus. Corticotropin-releasing hormone (CRH) deficiency, which is caused by defects in the synthesis or release of CRH, is a cause of secondary adrenocortical insufficiency. The clinical presentations are hypoglycemia, weight loss, anemia, weakness, nausea, vomiting and hyponatremia. Acquired CRH deficiency has also been suggested to occur based on a lack of adrenocorticotropic hormone (ACTH) response to insulin-induced hypoglycemia, but there is a normal ACTH response to exogenous CRH. We experienced a case of a woman with pituitary macroadenoma accompanied with CRH deficiency. We report here on this case with the review of the literature.



References
6. Verhelst J, Abs R. Hyperprolactinemia: pathophysiology and management. Treat Endocrinol. 2003. 2:23–32.
7. Arafah BM. Reversible hypopituitarism in patients with large nonfunctioning pituitary adenoma. J Clin Endocrinol Metab. 1986. 62:1173–1179.
8. Stacpoole PW, Interlandi JW, Nicholson WE, Ravin D. Isolated ACTH deficiency: a heterogeneous disorder. Critical review and report of four new cases. Medicine. 1982. 61:13–24.
9. Fehm HL, Voigt KH, Pfeiffer EF. Adrenocortical insufficiency as a result of isolated corticotropin-releasing hormone (CRH) deficiency. Dtsch Med Wochensch. 1973. 98:2066–2068.
11. Laron Z, Keret R, Bauman B, Pertzelan A, Ben-Zeev Z, Olsen DB, Comaru-Schally AM, Schally AV. Differential diagnosis between hypothalamic and pituitary hGH deficiency with the aid of synthetic GHRH 1-44. Clin Endocrinol. 1984. 21:9–12.
12. Woolf PD, Schalch DS. Hypopituitarism secondary to hypothalamic insufficiency. Ann Intern Med. 1973. 78:88–90.
13. Hermus AR, Pieters GF, Pesman GJ, Smals AG, Benraad TJ, Kloppenbong PW. ACTH and cortisol response to ovine corticotrophin-releasing factor in patients with primary and secondary adrenal failure. Clin Endocrinol. 1985. 22:761–769.
14. Schulte HM, Chrousos GP, Avgerinos P, Oldfild EH, Gold PW, Cutler GB Jr, Loriaux DL. The corticotropin-releasing hormone stimulation test: a possible aid in the evaluation of patients with adrenal insufficiency. J Clin Endocrinol Metab. 1984. 58:1064–1067.
15. Shibutani Y. Prolactin dynamics in a patient with isolated ACTH deficiency accompanied by hyperprolactinemia. Am J Med Sci. 1988. 295:140–143.
16. Nishihara E, Kimura H, Ishimaru T, Kiriyama T, Yokoyama N, Yamashita S, Nagataki S. A case of adrenal insufficiency due to acquired hypothalamic CRH deficiency. Endocr J. 1997. 44:121–126.
17. Schulte HM, Chrousos GP, Avgerinous P, Oldfield EH, Gold PW, Cutler GB Jr, Loriaux DL. The corticotropin releasing hormone test: a possible aid in the evaluation of patients with adrenal insufficiency. J Clin Endocrino Metab. 1984. 58:1064–1067.
18. Bohnet HG, Dahlen HG, Wuttke W, Schneider HPG. Hyperprolactinemic anovulatory syndrome. J Clin endocrinol Metab. 1975. 42:132–143.
19. Molitch ME, Elton RL, Blackwell RE, Caldwell B, Chang RJ, Jaffe R, Joplin G, Robbins RJ, Tyson J, Thorner MO. Bromocriptine as primary therapy for prolactin-secreting macroadenomas: results of a prospective multicenter study. J Clin Endocrinol Metab. 1985. 60:698–705.
20. Vance ML, Cragun JR, Reimnitz C, Chang RJ, Rashef E, Blackwell RE, Miller MM, Molitch ME. CV 205-502 treatment of hyperprolactinemia. J Clin Endocrinol Metab. 1989. 68:336–339.
 XML Download
XML Download