

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Multiple endocrine neoplasia I (MEN I) is a genetic disorder that consists of neoplasia of neuroendocrine type in the parathyroid glands, in the islets of Langerhans in the pancreas, and in the anterior pituitary gland. Primary hyperparathyroidism is the most common feature and occurs in approximately 95% of MEN I patients. Pancreatic islet cell tumors occur in 40% of MEN I patients. Most of these tumors produce excessive amounts of hormones, such as gastrin, insulin, glucagon and vasoactive intestinal polypeptide (VIP). VIP-producing pancreatic tumors (VIPoma) associated with MEN I are rare and so far only one has been reported in Korea.
Recently, we came across a case of MEN I, associated VIPoma presented persistent hypercalcemia after a parathyroidectomy. A 70 year old man had suffered from large amount of watery diarrhea, severe general weakness and paralysis of lower limbs for 3 months which suggests symptoms of hypercalcemia. Before the patient visited our hospital, he underwent subtotal parathyroidectomy due to hyperparathyroidism. Even though he was operation, there was no subsidization of the symptoms and abnormal findings of blood chemistry such as hypercalcemia, hypocalemia were remained unchanged. However, the parathyroid hormone level was still within normal limits. Abdominal computerized tomography scan demonstrated a mass of 2.5 cm diameter in tail of the pancreas. As serum level of VIP hormone was also elevated, distal pancreatectomy was carried out to performed.
There was improvement in the symptoms towards the normal condition and the level of biochemical parameters such as serum potassium, calcium and VIP, were also within the normal limits. In a direct sequence analysis, GAC → CAT (Asp → His) point mutation, at codon 383 of exon 9 of the MEN I gene was identified in both the patient and his son.
The authors report a rare case of VIPoma associated with MEN I with review of literature on MEN I.
Figures and Tables
Fig. 1
201Tl-99mTc subtraction images show enlargement of the lower part of the right parathyroid gland

Fig. 2
Computerized tomography scan of the abdomen shows about 2.5 cm sized well defined mass lesion in the pancreatic tail portion
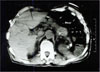
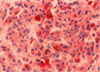
Fig. 3
Gross finding of the distal pancreatectomy. External surface shows partly encapsulated tumor mass by thin fibrous tissue


References
1. Erdheim J. Zur normalen und pathologicxchen histology der glandula thyroidea und Hypophysis. Beitr Pathol Anat. 1903. 33:158–161.
2. Underdahl LO, Woolner LB. Multiple endocrine adenomas. Report of eight cases in which parathyroids, pituitary, and pancreatic islets were involved. J Clin Endoclinol. 1953. 13:20–47.
6. Chandrasekharappa SC, Guru SC, Manickam P, Olufemi SE, Collins FS, Emmert-Buck MR, Debelenko LV, Zhuang Z, Lubensky IA, Liotta LA, Crabtree JS, Wang Y, Roe BA, Weisemann J, Boguski MS, Agarwal SK, Kester MB, Kim YS, Heppner C, Dong Q, Spiegel AM, Burns AL, Marx SJ. Positional cloning of the gene for multiple endocrine neoplasia type 1. Science. 1997. 276:404–407.
7. Ballard HS, Frame B, Hartstock C. Familial multiple endocrine adenoma-peptic ulcer complex. Medicine. 1964. 43:481–515.
8. Gelston AL, Delishe MB, Patel YC. Multiple endocrine adenomatosis type 1 occurrence in an octogenarian with high levels of circulating pancreatic polypeptide. JAMA. 1982. 247:665–666.
9. Marx SJ. Vogelstein B, Kinzler KW, editors. Multiple endocrine neoplasia type 1. Genetic Basis of Human Cancer. 1998. New York: McGraw Hill;489–506.
10. Benson L, Ljunghall S, Akerstrom G, Oberg K. Hyperparathyroidism presenting as the first lesion in multiple endocrine neoplasia type 1. Am J Med. 1987. 82:731–737.
11. Eberle F, Grun R. Multiple endocrine neoplasia type l (MEN-1). Ergbeg inn Med Kinderheilkd. 1981. 46:76–149.
12. Brandi ML, Marx SJ, Aubach GD, et al. Familial multiple endocrine neoplasia type 1: A new look at pathophysiology. Endocr Rev. 1987. 8:391–412.
13. Christensson T. Familial hyperparathyroidism. Ann lntern Med. 1976. 85:614–615.
14. Brown CH, Crile G Jr. Pancreatic adenoma with intractable diarrhea, hypokalemia and hypercalcemia. JAMA. 1964. 190:30–34.
15. Burkhardt A. Das Verner-Morrison Zyndrome. Klin Pathol Anat Klin Wochenschr. 1976. 54:1–11.
16. Verner JV, Morrison AB. lslet cell tumor and a syndrome of refractory water diarrhea and hypokalemia. Am J Med. 1958. 25:374–380.
17. Marks IN, Bank S, Louw JH. lslet cell tumor of the pancreas with reversivle watery diarrhea and achlortydria. Gastroenterology. 1967. 52:695–708.
18. Matsumoto KK, peter JB, Schultze RG, Hakim AA, Franck PE. Watery diarrhea and hypokalemia associated with pancreatic islet cell adenoma. Gastroenterology. 1966. 50:231–242.
19. Bloom SR, Polak JM, Pearse AGE. Vasoactive intestinal peptide and watery diarrhea syndrome. Lancet. 1973. 2:14–16.
20. Verner JV, Morrison AB. Endocrine pancreatic islet disease with diarrhea: report of a case due to diffuse hyperplasia of non beta islet tissue with a review of 54 additional cases. Arch lntern Med. 1974. 133:492–500.
21. Kofstad J, Froyshov I, Gjone E, Blix S. Pancreatic tumor with intractable watery diarrhea, hypokalemia and hypercalcemia. Electrolyte valance studies. Scand J Gastroenterol. 1967. 2:246–251.
22. Hohmann EL, Levine L, Tashjian AH. Vasoactive intestinal peptide stimulates bone resorption via a cyclic adenosine 3'-, 5'-morphosphate-dependent mechanism. Endocrinology. 1983. 112:1233–1239.
23. Krejs GJ. VIPoma Syndrome. Am J Med. 1987. 82:Suppl. 5B. 37–48.
24. Kahn CR, Levy AG, Gardner JD, Miller JV, Gordon P, Schein PS. Pancreatic cholera: beneficial effects of treatment with streptozotocin. N Engl J Med. 1975. 292:859–945.
25. Charleux H. Syndrome de Vermer Morrison, Cholera endocrine au vipome. La Nouv Presse Med. 1982. 11:859–862.
26. Krejs GJ. Bloom SR, Polak JM, editors. Peptidergic control of intestinal secretion-studies in man. Gut hormes. 1981. 2nd ed. Edinburgh: churchill Livingstone;516–520.
27. Ruskone A, Rene E, Chayvialle JA, et al. Effect of somatostatin on diarrhea and small intestinal water and electrolyte transport in a patient with pancreatic cholera. Dig Dis Sci. 1982. 27:459–466.
28. Moertel CG, Hanley JA, Johnson LA. Streptozocin alone compared with streptozocin plus fluorouracil in the treatment of advanced islet-cell carcinoma. N Engl J Med. 1980. 303:1189–1194.
29. Larsson C, Skogseid B, Oberg K, et al. Multiple endocrine neoplasia type I gene maps to chromosome 11 and is lost insulinoma. Nature. 1988. 332:85–87.
30. Debelenko LV, Emmert Buck MR, Maickam P, et al. Haplotype analysis defines a minimal interval for the multiple endocrine neoplasia typ 1(MEN) gene. Cancer Res. 1997. 57:1039–1042.
31. Agarwal SK, Kester MB, Debelenko LV, et al. Germline mutations of the MEN1 gene in familial muliple endocrine neoplasea type 1 and related states. Hum Mol Genet. 1997. 6:1169–1175.
 XML Download
XML Download