

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Acute suppurative thyroiditis is an uncommon disease, which usually affects patients with pre-existing thyroid gland pathology. Here, a case of thyroid abscess associated with lymphocytic thyroiditis, was experienced in a 35-year-old female. She had a fever, chill, sore throat and tenderness in the area of the left thyroid of 10 days duration. She visited our hospital due to her persistent sore throat, which did not subside after antibiotics treatment for 5 days. On neck ultrasonography, a heterogeneous nodule (1.3×1.5×2.1 cm) in the right lobe and cyst-like nodule (1.8×1.5×2.8 cm) in the left lobe of the thyroid were found. The thyroid gland showed slightly increased, uneven uptake of Tc-99m on a thyroid scan. Pus-like fluid aspirated from the left nodule showed numerous neutrophils and necrotic materials on cytological examination. Abundant lymphocytes were found in aspirates from the right thyroid nodule. Neither a finding suggestive of pyriform sinus nor other anomaly was discovered in the neck CT scan and UGI series. After further antibiotic treatments for 2 weeks, the inflammatory symptoms and thyroid tenderness completely subsided. However, the nodule in the right lobe of the thyroid was still palpable, but without tenderness when examined after 4 weeks.
Figures and Tables

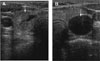 | Fig. 2Thyroid ultrasonography shows a heterogenous, hypoechoic mass (arrow) with central anechoic area in the right lobe of the thyroid gland (A) and a cyst (arrow) with posterior acoustic enhancement in the left lobe of the thyroid gland (B).
|


References
1. Pearce EN, Farwell AP, Braverman LE. Thyroiditis. N Engl J Med. 2003. 348:2646–2655.
3. Altemeier WA. Acute pyogenic thyroiditis. Arch Surg. 1950. 61:76–85.
4. Farwell AP. Braverman LE, Utiger RD, editors. Subacute thyroiditis and acute infectious thyroiditis. Werner & Ingbar's The Thyroid: A Fundamental and Clinical Text. 9th ed. Philadelphia: Lippincott Williams & Wilkins;536–547.
5. Sun JH, Chang HY, Chen KW, Lin KD, Lin JD, Hsueh C. Anaerobic thyroid abscess from a thyroid cyst after fine-needle aspiration. Head Neck. 2002. 24:84–86.
7. Myssiorek D, Lee J, Shikowitz M, Sarnataro R. Immobile vocal fold secondary to thyroid abscess: a case report. Ear Nose Throat J. 2000. 79:453–455.
8. Kawanaka M, Sugimoto Y, Suehiro M, Fukuchi M. Thyroid imaging in a typical case of acute suppurative thyroiditis with abscess formation due to infection from a persistent thyroglossal duct. Ann Nucl Med. 1994. 8:159–162.
9. Larsen PR, Davies TF. Larsen PR, Kronenberg HM, Melmed S, Polonsky KS, editors. Hypothyroidism and Thyroiditis. Williams Textbook of Endocrinology. 10th ed. Philadelphia: Sauders;423–455.
13. Soderstrom N. Puncture of goiters for aspiration biopsy. Acta Med Scand. 1952. 144:237–244.
14. Friedman M, Shimaoka K, Rao U, Tsukada Y, Gavigan M, Tamura K. Diagnosis of chronic lymphocytic thyroiditis (nodular presentation) by needle aspiration. Acta Cytol. 1981. 25:513–552.
 XML Download
XML Download