

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
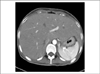
When a patient with diabetes presents with hepatomegaly and increased level of liver enzymes, glycogenosis or nonalcoholic steatohepatitis (NASH) should be considered.
Glycogenosis is mainly developed in patients with type 1 diabetes, when blood glucose level is poorly controlled, when a high dosage of insulin is administered in ketoacidosis, or when glucose is given to control hypoglycemia caused by high dosage of insulin. On the other hand, the main causes of NASH, which are known to mainly affect type 2 diabetes patients, are obesity, dyslipidemia or insulin resistance. Glycogenosis differs from NASH, the former being a reversible change that improves with the control of blood glucose level and the minimum dosage requirement of insulin, and the latter being a progressive disease that may lead to fibrosis or cirrhosis of the liver. However, clinical differentiation of the two diseases is difficult and liver biopsy is helpful for making a definite diagnosis.
We present a type 1 diabetes patient with poorly controlled blood glucose level, who have had a frequent history of diabetic ketoacidosis, showing hepatomegaly and a slight increase in liver enzyme level. The patient was diagnosed as diabetic glycogenosis, confirmed by liver biopsy. Strict control of the blood glucose level resulted in rapid improvement showing the reversible nature of the disease.
Figures and Tables


References
1. Goodman JI. Hepatomegaly and diabetes mellitus. Ann Intern Med. 1953. 39:1077–1087.
2. Van Steenbergen W, Lanckmans S. Liver disturbances in obesity and diabetes mellitus. Int J Obes Relat Metab Disord. 1995. 19(S3):S27–S36.
3. Mauriac P. Gros ventre, hepatomegalie, troubles de la croissance chez les enfants diabetiques traites depuis plusieurs annes par l'insuline. Gaz Hebd Med Bourdeaux. 1930. 26:402–410.
5. Chatila R, West AB. Hepatomegaly and abnormal liver tests due to glycogenosis in adults with diabetes. Medicine. 1996. 75:327–333.
6. Munns CF, McCrossin RB, Thomsett MJ, Batch J. Hepatic glycogenosis: reversible hepatomegaly in type 1 diabetes. J Paediatr Child Health. 2000. 36:449–452.
7. Nakamuta M, Ohashi M, Goto K, Tanabe Y, Hiroshige K, Nawata H. Diabetes mellitus-associated glycogen storage hepatomegaly: report of a case and review of the Japanese literature. Fukuoka Igaku Zasshi. 1993. 84:354–358.
8. Stone BG, Van Thiel DH. Diabetes mellitus and the liver. Semin Liver Dis. 1985. 5:8–28.
9. Olsson R, Wesslau C, William-Olsson T, Zettergren L. Elevated aminotransferases and alkaline phosphatases in unstable diabetes mellitus without ketoacidosis or hypoglycemia. J Clin Gastroenterol. 1989. 11:541–545.
10. Manderson WG, McKiddie MT, Manners DJ, Stark JR. Liver glycogen accumulation in unstable diabetes. Diabetes. 1968. 17:13–16.
11. Yu YM, Howard CP. Improper insuline compliance may lead to hepatomegaly and elevated hepatic enzymes in type 1 diabetic patients. Diabetes Care. 2004. 27:619–620.
12. Wolfsdorf JI, Weinstein DA. Glycogen storage diseases. Rev Endocr Metab Disord. 2003. 4:95–102.
13. Lee RG. Nonalcoholic steatohepatitis: a study of 49 patients. Hum Pathol. 1989. 20:594–598.
14. Younossi ZM, Gramlich T, Matteoni CA, Boparai N, McCullough AJ. Nonalcoholic fatty liver disease in patients with type 2 diabetes. Clin Gastroenterol Hepatol. 2004. 2:262–265.
 XML Download
XML Download