

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Since 1911, when Leonhard Noon and John Freeman introduced allergen-specific immunotherapy (AIT), evidence suggesting its efficacy for various allergens has accumulated. The duration of conventional AIT, including subcutaneous immunotherapy (SCIT) and sublingual immunotherapy (SLIT), is 3–5 years, which requires a large commitment of time, money, and effort from patients. Moreover, many patients experience local or systemic adverse effects, with those receiving SLIT reporting abdominal discomfort and itching or burning sensations in the oral cavity, and those treated with SCIT experiencing pain at the injection site, urticaria, and even systemic reactions, including anaphylaxis. For these reasons, AIT is generally regarded as a second- or third-line therapy and is thus recommended only to patients whose allergic symptoms are not sufficiently alleviated by pharmacotherapy and allergen avoidance or in whom pharmacotherapy is not feasible because of its side effects, contraindications, patient preference, or other reasons. Consequently, <5% of allergy patients are treated with AIT, although its therapeutic effects persist for several years. To treat allergic diseases more vigorously and reduce their social burden, therapeutic modalities that overcome the limitations of conventional AIT are needed.
Go to : 
INTRANODAL INJECTION IN ALLERGEN-SPECIFIC IMMUNOTHERAPY
More than a decade ago, Kündig and colleagues [12345678] proposed the geographical concept of immunogenicity. T and B cells can recognize a nearly unlimited number of antigens via their diverse repertoire of receptors, which reflect random rearrangements of their receptors during lymphocyte development. An adaptive immune response to a specific antigen occurs only after an antigen has encountered millions of T and B cells, because an antigen is recognized by only 1 in 107 of these cells. To enhance the possibility that antigens meet their specific T and B cells, they are drained into the lymph nodes, which are rich in both cell types. However, oligopeptides and proteins are not effectively concentrated in the lymph nodes, which accumulate only a small fraction of an injected dose (10−6 of an oligopeptide and 10−3 of a protein dose) [4]. For this reason, allergen extracts or recombinant allergens that consist mainly of peptides and proteins remain largely outside the lymphoid organs and, thus, cannot effectively stimulate the adaptive immune system in conventional AIT. Because of these low levels of efficacy, multiple doses and prolonged therapy may be required. To overcome the shortcomings of conventional AIT, Senti et al. [9] introduced intralymphatic immunotherapy (ILIT) as a new approach to AIT in 2008.
Go to :
LITERATURE SEARCH
We performed a literature review to examine the treatment efficacy and adverse effects of ILIT. The PubMed databases were searched to identify human clinical trials or animal studies of ILIT. The search was updated until June 2017, and the publication language was not restricted.
Go to :
CLINICAL TRIALS OF INTRALYMPHATIC IMMUNOTHERAPY
Since the first study performed by Senti et al., 8 clinical trials have evaluated the clinical efficacy and adverse effects of ILIT [910111213141516]. Their results are summarized in Table 1. In the initial study performed by Senti et al. [9], 165 patients with grass-pollen-induced rhinoconjunctivitis were randomly assigned to receive either 54 subcutaneous injections with pollen extract over 3 years (cumulative allergen dose: 4,031,540 standardized quality units [SQ-U] of Alutard SQ, ALK-Abelló, Hørsholm, Denmark) or 3 intralymphatic injections over 2 months (cumulative allergen dose: 3,000 SQ-U of Alutard SQ). Nasal reactivity, assessed using the nasal allergens provocation test (NAPT), decreased within 4 months in the ILIT group, which also showed long-lasting tolerance that was similar to that in the SCIT group. ILIT also alleviated hay fever symptoms and reduced both skin reactivity in the skin prick test (SPT) and the serum level of allergen-specific IgE. The side effects of ILIT were restricted to mild pain that was less than that of venous puncture. No moderate-to-severe systemic adverse reactions were provoked; only mild ones that were fewer in number than those induced by SCIT were observed. Senti et al. [10] conducted a subsequent, randomized double-blind ILIT trial in patients with cat allergies using a modular antigen transporter (MAT) vaccine (MAT-Fel d 1) generated from a recombinant major cat-dander allergen (Fel d 1) fused to a translocation sequence and to part of the human invariant chain. ILIT with MAT-Fel d 1 elicited fewer adverse events and a higher level of nasal tolerance than observed in the placebo group. ILIT with MAT-Fel d 1 also stimulated regulatory T-cell responses and increased cat-dander-specific IgG4 levels, with both correlating positively with interleukin (IL)-10 production.
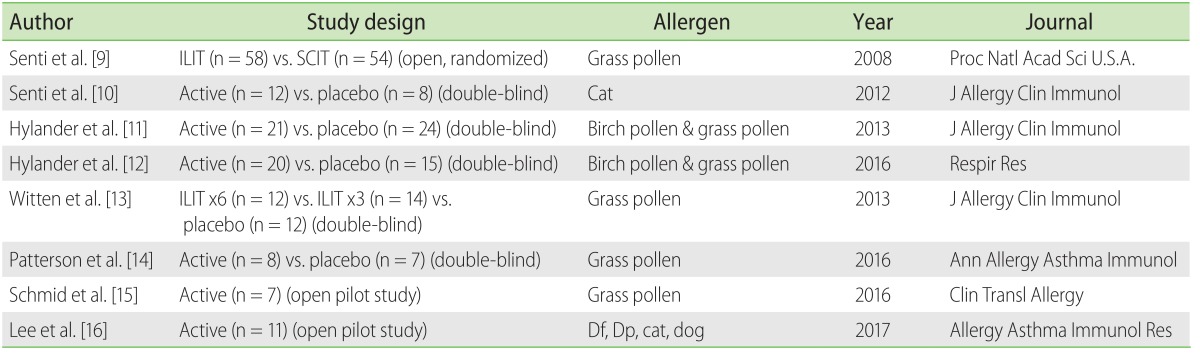
Table 1
Clinical trials of intralymphatic immunotherapy
Intralymphatic injections were administered 3 times at 4-week intervals in all but one study, by Witten et al. [13].
ILIT, intralymphatic immunotherapy; SCIT, subcutaneous immunotherapy; Df, Dermatophagoides farina; Dp, Dermatophagoides pteronyssinus.
![]()
In 2013, Hylander et al. [11] reported—first in a pilot study and subsequently in a double-blind placebo-controlled trial—the highly efficient therapeutic effects and safety of ILIT in patients with pollen-induced allergic rhinitis. The 21 patients with allergic rhinitis received 3 intralymphatic inguinal injections of either ALK-Abelló Alutard (containing 1,000 SQ-U birch pollen or grass pollen) or placebo. ILIT did not provoke any severe adverse events, but it did improve seasonal allergic symptoms. Decreases in both nasal reactivity in the NAPT and nasal inflammation were also observed. These improvements in clinical and laboratory parameters were not observed in the placebo group. The authors again conducted further double-blind placebo-controlled trials with birch- or grass-pollen vaccine (Alutard) and confirmed the efficacy and safety of ILIT [12].
However, Witten et al. [13] questioned the efficacy of ILIT based on the results of their double-blind, placebo-controlled study. The 45 adult patients with grass-pollen-induced rhinoconjunctivitis were randomly allocated to 1 of 3 groups receiving 6 injections of 1000 SQ-U of alum-adsorbed Phleum pratense (x6 group), 3 injections of 1000 SQ-U followed by 3 injections of placebo (x3 group), or 6 injections of placebo. As indicated by the combined mean symptom and medication score (SMS) for the entire grass-pollen season, ILIT failed to demonstrate significant clinical efficacy in the 38 patients available for evaluation. Moreover, the x3 group had a slightly negative outcome, with a 12% higher total SMS than the placebo group during the entire grass-pollen season. During the peak season, the SMS was higher in both treatment groups than in the placebo group. Additionally, the 2 ILIT groups showed no significant change in the global assessment or rhinitis-related quality of life (RQLQ) scores compared to the placebo group, which improved significantly from pretreatment to posttreatment.
In 2016, Patterson et al. [14] reported the results of a randomized, double-blind, placebo-controlled, parallel-group pilot study in which American adolescents and young adults received ILIT. In their study, 7 patients were randomized to active treatment with 20,000 PNU aluminum hydroxide adsorbed grass pollen extract (Center-Al Phleum pratense; ALK, Round Rock, TX, USA)/mL, and 8 patients received injections of diluent (normal saline with phenol). Study participants received 3 preseasonal, escalated-dose inguinal lymph node injections (0.1, 0.2, and 0.5 mL) of either placebo or study extract at least 4 weeks apart. Adverse reactions were comparable between the 2 groups such that the mean overall total safety score was similar between the active treatment and placebo groups. With regards to therapeutic efficacy, the mean total combined scores were lower in the pollen-treated than in the placebo groups throughout the pollen season and during the peak pollen period.
Schmid et al. [15] recently reported an open trial of ILIT in 7 patients with allergic rhinoconjunctivitis due to grass. In their study, allergen (0.1-mL Alutard Phleum pratense, 10,000 SQU/mL, ALK-Abelló) was injected into the inguinal lymph nodes 3 times at monthly intervals. The SMSs of these patients were reduced after 3 injections, whereas their RQLQ scores from 2013 were comparable to those of previous seasons. Furthermore, tolerance of grass pollen increased significantly according to the NAPT as well as the titrated SPT, performed before ILIT and after the ensuing grass-pollen season. In addition to those in vivo tests, after ILIT, an increase in the serum level of grass-allergen-specific plasmablasts expressing isotypes other than IgE was determined.
All of the aforementioned studies of ILIT reported its safety as a new modality of AIT and the absence of serious local or systemic reactions. However, in 2017, we determined that moderate-to-severe local or systemic hypersensitivity reactions, including anaphylaxis, could be provoked by ILIT when aqueous allergen extracts were used [16]. In our study, 11 patients with allergic rhinitis who were sensitized to Dermatophagoides farinae (Df), Dermatophagoides pteronyssinus (Dp), cat, and/or dog allergens received three intralymphatic inguinal injections of sensitized allergen extract (HollisterStier, New Orleans, LA, USA). Rhinitis symptoms were alleviated and quality of life was improved 4 months after ILIT, with both improvements lasting for 1 year after treatment. Additionally, reductions in the nasal reactivities to Df or Dp allergen, as assessed by the NAPT, were documented after ILIT in patients allergic to Df or Dp. Whereas skin reactivity to allergens in the SPT was generally increased after ILIT, the difference did not reach statistical significance. However, there were 2 cases of anaphylaxis, 1 case of a moderate-to-severe systemic hypersensitivity reaction and one of a large local reaction at the injection site, after ILIT. Based on these results, we proposed that: (1) SPTs should be performed with serial dilutions of allergens, (2) the initial dose of the allergens in ILIT should not exceed the maximal concentration leading to an allergen/histamine ratio for wheals of <1, and (3) patients undergoing ILIT with allergens at doses exceeding this concentration should be carefully monitored.
Go to :
INTRALYMPHATIC IMMUNOTHERAPY IN ANIMAL STUDIES
In contrast to human trials, there have been relatively few animal studies of ILIT (Table 2). In 2008, Martínez-Gómez et al. [17] reported the results of murine experiments. Female cytometric bead array (CBA) mice were immunized 3 times at 2-week intervals by injection with the major bee venom allergen phospholipase A2 (n = 5) or the major cat allergen recombinant Fel d 1 (n = 4). The direct injection of these allergens into the inguinal lymph nodes stimulated allergen-specific IgG and T-cell responses in addition to enhancing the production of IgG2a that protected against allergen-induced anaphylaxis. The same report included biodistribution studies suggesting the delivery of antigens into lymph nodes is more effective than subcutaneous injection.
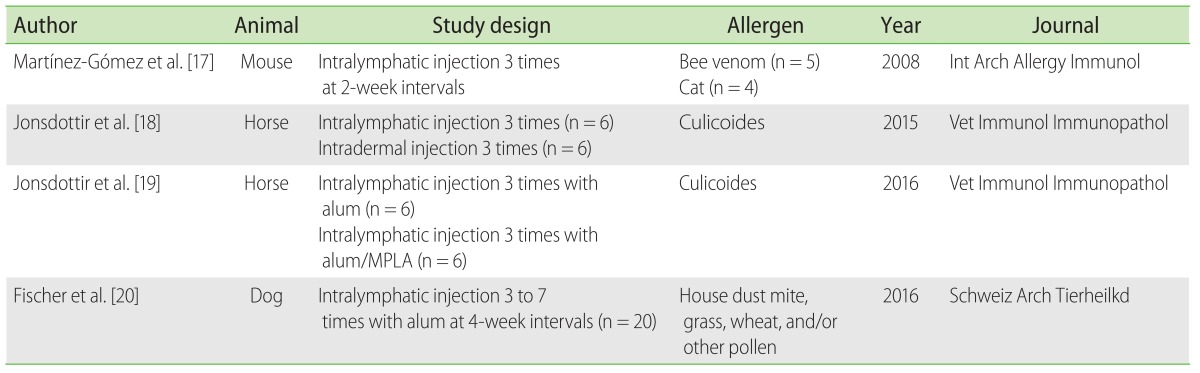
In addition to translational research, there have been several veterinary studies. In 2015, Jonsdottir et al. [18] reported a pilot study of ILIT against insect-bite hypersensitivity (IBH) in horses. IBH is an allergic dermatitis of horses caused by the bites of midges (Culicoides spp.). It does not occur in Iceland, where these insects are absent but develops with a high frequency in Icelandic horses exported to mainland Europe, where Culicoides is present. The authors hypothesized that immunization with Culicoides allergens before export would reduce the incidence of IBH in exported Icelandic horses. Twelve horses were vaccinated three times with 10 µg of each of the four recombinant Culicoides nubeculosus allergens (r-allergens). Six horses were injected intralymphatically and 6 intradermally, but neither group showed IgE-mediated reactions. Specifically, the horses did not respond to Culicoides extract stimulation in a sulfidoleukotriene release test nor did they develop a relevant immediate hypersensitivity reaction to the r-allergens in the skin test. Although intralymphatic injection was slightly more efficient than intradermal injection, the difference was not significant. Neither route of vaccination with r-allergens provoked adverse effects in the tested horses.
One year later, the same authors reported that, in another study, horses intralymphatically injected with r-allergens in aluminum hydroxide (alum) or in alum/monophosphoryl lipid A also did not show IgE-mediated reactions [19]. However, a critical limitation of both studies was that they did not determine whether intralymphatic or intradermal vaccination actually prevented IBH after the horses were exported to Europe. In 2016, Fischer et al. [20] reported the results of an ILIT study against canine atopic dermatitis. Twenty atopic dogs underwent ILIT with alum-precipitated allergens injected into the popliteal lymph node every 4 weeks for a total of 3 to 7 times. A good clinical response was obtained in 12 of 20 dogs (60%), with improvement seen in some of them after 4 weeks. However, because this study did not have control groups, it could not validate the efficacy of ILIT against canine atopic dermatitis. Randomized placebo-controlled, blind trials are also needed in veterinary research to elucidate the efficacy of ILIT.
Go to :
MECHANISM OF INTRALYMPHATIC IMMUNOTHERAPY
As in previous studies of conventional AIT, many clinical trials have evaluated whether ILIT alleviates allergic inflammation by inhibiting Th2 immunity and by enhancing Th1 or regulatory T cell (Treg) responses. In their first published study of ILIT, Senti et al. [9] reported reduced serum levels of allergen-specific IgE and skin reactivity to allergens in a skin test. They subsequently reported ILIT-induced increases in allergen-specific IgG4 in the serum of patients and the in vitro production of IL-10 in peripheral blood mononuclear cells (PBMCs) stimulated with allergens. Moreover, the 2 findings were correlated with each other [10]. However, in the study conducted by Hylander et al. [11], serum allergen-specific IgE was increased and serum allergen-specific IgG4 was unchanged after ILIT. They also reported no significant change in serum allergen-specific IgE or IgG4 in patients undergoing ILIT, but a significantly increased allergen-specific IgG4 affinity was observed in symptomatically improved patients [12]. In the study of Witten et al. [13], both serum allergen-specific IgE and IgG4 were increased after ILIT. Moreover, IL-4 and IL-10 production, as well as the expression of FoxP3 increased, whereas interferon (IFN)-γ production by stimulated PBMCs decreased after ILIT. In our study, serum allergen-specific IgE and IgG4 increased 4 months after ILIT, but they had decreased by 1 year later [16]. Skin reactivities to allergens were also prone to increase after ILIT. In their pilot study of allergen-specific plasmablasts, Schmid and colleagues reported increases in the subset of cells expressing isotypes other than IgE after ILIT [15].
In a murine model, Martínez-Gómez et al. [17] showed increases in serum allergen-specific IgG1 and IgG2a rather than IgE after ILIT, as well as elevated levels of cytokines, including IFN-γ, IL-10, IL-2, and IL-4, in splenocytes stimulated with allergens in vitro.
Veterinary research performed by Jonsdottir et al. [1819] found increased serum levels of allergen-specific IgG in the absence of the production of allergen-specific IgE; this study also reported that IgG antibodies could partly block the r-allergen-binding of serum IgE from an IBH-affected horse, as demonstrated in a blocking activity test. The same authors showed that IgG antibodies bound to protein bands on blots of C. nubeculosus salivary gland extract and that allergen-stimulated PBMCs from horses treated with ILIT produced significantly more IFN-γ and IL-10 than control horses [19].
Based on these human and animal studies of ILIT, especially the results of Schmid et al. [15] in their study of plasmablasts, the sequence of events that occurs in lymph nodes injected with allergens can be predicted (Fig. 1). First, a naïve B cell entering the lymph node through an afferent lymphatic vessel undergoes clonal expansion and somatic hypermutation in the dark zone of the germinal center. Allergens injected into a lymph node are phagocytosed by follicular dendritic cells, and their peptides are presented on major histocompatibility complex class II molecules to B cells in the light zone of the germinal center. These B cells are activated and differentiate into plasmablasts, plasma cells, and memory B cells, after which they exit the lymph node through the medulla and an efferent lymphatic vessel. They may secrete allergen-specific IgE, IgG4, or other antibody isotype with or without enhanced affinity. However, the mechanism of ILIT, especially the roles of Th1, Th2, and Treg immunity, remains to be investigated.
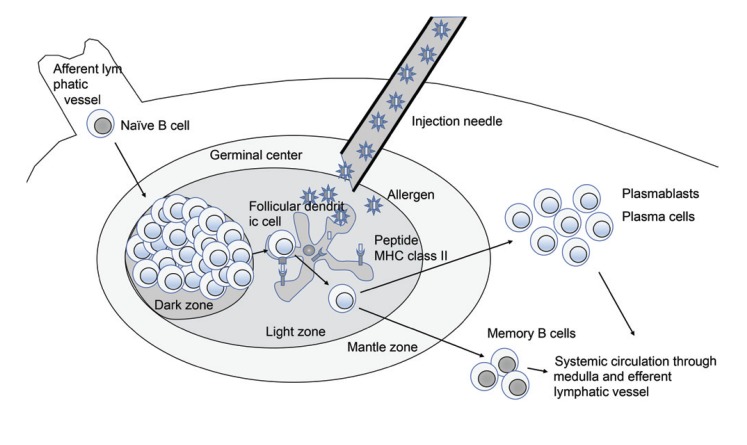 | Fig. 1Possible mechanism of immune modulation in intralymphatic immunotherapy. After entering the lymph node through an afferent lymphatic vessel, a naïve B-cell undergoes clonal expansion and somatic hypermutation within the dark zone of the germinal center. Allergens injected into a lymph node are phagocytosed by follicular dendritic cells, and their peptides are presented on major histocompatibility complex (MHC) class II molecules to B cells within the light zone of the germinal center. These activated B cells differentiate into plasmablasts, plasma cells, and memory B cells. They then exit the lymph node through the medulla and efferent lymphatic vessels. The circulating B cells, with or without enhanced affinity, may secrete allergen-specific IgE, IgG4, or other antibody isotype.
|
Hypersensitivity reactions have been attributed to the possible leakage of intralymphatically injected allergens from the lymph node (Fig. 2). However, the lymph nodes are not isolated; as mentioned above, they are connected to the systemic circulation through the medulla, arteries, veins, and lymphatic vessels. These connections allow injected allergens to exit a lymph node and reach the systemic circulation, where they provoke hypersensitivity reactions. Note that even allergens at very low concentrations that rarely cause a severe hypersensitivity reaction in SCIT can provoke anaphylaxis when intralymphatically injected, as demonstrated in our previous study [16].
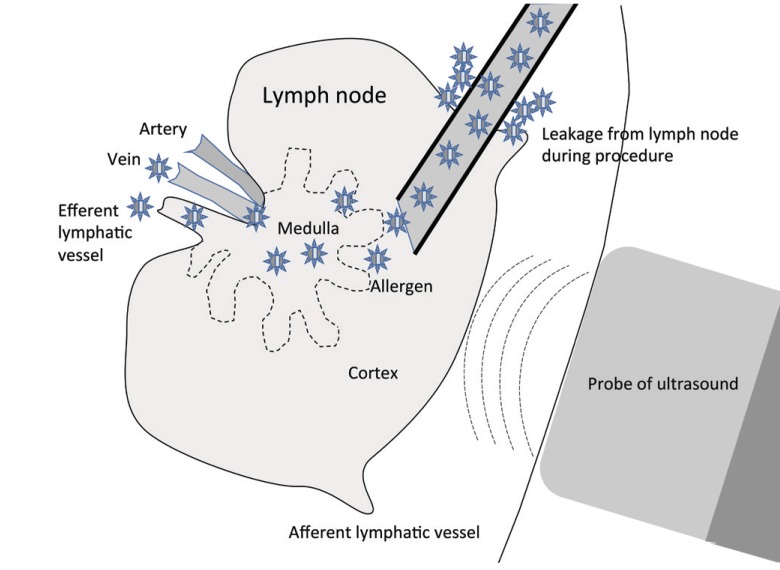 | Fig. 2Possible mechanism underlying the development of a hypersensitivity reaction in intralymphatic immunotherapy. Although we performed ultrasound-guided intralymphatic injection after confirming the targeted lymph node, small amount of allergens can be leaked from lymph node during the procedure and this may lead to systemic hypersensitivity reaction. In addition, the lymph node is not isolated but connected to the systemic circulation through the medulla, arteries, veins, and the lymphatic vessels. Therefore, allergens injected into a lymph node can use this route to reach the systemic circulation and provoke a hypersensitivity reaction.
|
Go to :
SUMMARY
Recent clinical trials of ILIT against allergic rhinitis have examined its ability to overcome the limitations of the prolonged treatment duration and local or systemic hypersensitivity reactions that characterize conventional AIT, including SCIT and SLIT. Most of these studies demonstrated the rapid onset and long duration of the therapeutic effects as well as the absence of serious adverse effects. However, one study raised questions about the therapeutic efficacy of ILIT, and another reported moderate-to-severe local and systemic hypersensitivity reactions, including anaphylaxis, after ILIT.
ILIT has also been studied in animals, in the form of translational and veterinary research. In the former, the mechanism, efficacy, and adverse effects of ILIT were evaluated in mice immunized by inguinal lymph node injection of the major bee venom allergen or the major cat allergen. In other veterinary studies, the utility of ILIT was evaluated in susceptible to IBH and in dogs with atopic dermatitis.
Despite several attempts to elucidate the mechanism, therapeutic efficacy, and adverse effects of ILIT, much remains to be learned.
Go to :
 XML Download
XML Download