

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Allergic rhinitis (AR) is a chronic inflammatory disease with a high and increasing prevalence, which has a significant impact on the quality of life (QoL), especially in children and young adults [1]. Failure to adequately treat AR may lead to a variety of comorbidities including asthma, sinusitis, otitis media, frequent respiratory infections, and orthodontic malocclusions, all of which may further impair health related quality of life (HRQoL) [23]. Therefore, unlike many other diseases whose goal of treatment may be centered on preventing death or future morbidity, the goal of treatment of AR is to improve a patient's well-being, or QoL [4].
A variety of validated and standardized questionnaires have been developed to evaluate HRQoL. The rhinoconjunctivitis quality of life questionnaire (RQoLQ) is one of the most widely used rhinitis-specific questionnaires. It covers 7 dimensions of health: sleep, nonnasal symptoms, practical problems, nasal symptoms, ocular symptoms, specific activities limited by symptoms in the previous week, and emotional function. However, similar symptoms may vary in their effect on different individuals, and individual QoL domains and individual symptoms may not equally correlate [5]. Some patients might be impaired by only a few nasal symptoms, whereas others might be less impaired by the same symptoms or more severe symptoms.
There are various phenotypes or inflammatory subtypes of AR. Nasal hyperreactivity to specific or nonspecific provocative agents is a principal feature of AR [6]. Nasal provocation tests with different provocative agents may reflect different aspects of the nasal inflammatory process [7], and has been used to assess the onset, effectiveness and tolerability of therapy [8].
However, the correlations of nasal responses to LTD4 and histamine nasal provocation with health related QoL assessed by RQoLQ in AR have not been evaluated and clarified. Consequently, the aim of this study was to analyze the correlations of LTD4 and histamine nasal challenges induced nasal symptoms and responsiveness with QoL in AR
MATERIALS AND METHODS
Study design
This is a cross-over study conducted on a random sample of college students in the colleges of Guangzhou in Southern China, between October 2012 and March 2013. Participants completed the RQoLQ [9], underwent skin prick tests (SPTs) to a panel of aeroallergens, and randomly underwent LTD4 and histamine nasal provocation in a 2-week interval. The study was approved by the Ethics Committee of First Affiliated Hospital of Guangzhou Medical University (approval number: 2012-18) and registered at ClinicalTrials.gov (NCT01963741) and. Written informed consent was signed by each participant.
Skin prick test
SPTs were performed with a panel of aeroallergens, as well as positive and negative controls (ALK, Hórsholm, Denmark). Allergic sensitization was defined as the presence of positive to at least one allergen. Allergens were grouped in perennial (Dermatophagoides pteronyssinus, Dermatophagoides farinae, Blomia tropicalis, Dog and Cat dander, Blattella germanica, Alternaria, Birch and Ragweed).
Quality of life
QoL was assessed by using the RQoLQ, which covers seven dimensions of health: sleep, nonnasal symptoms, practical problems, nasal symptoms, eye symptoms, activities limited by symptoms, and emotional function is one of the most widely used rhinitis-specific questionnaires. The self-administered questionnaire was completed by each participant. The severity of each item was rated range from 0 (not troubled) to 6 (extremely troubled). The mean value for each dimension and the overall health related QoL (HRQoL) (expressed as the mean of the seven dimension scores) were calculated [9].
Total symptom score 4
The patients recorded symptom severity in a form for four typical AR nasal symptoms: sneezing, rhinorrhea, nasal pruritus, and nasal congestion. A score ranging from 0 to 3 was used for each symptom: 0, no symptoms; 1, mild symptoms (symptoms clearly present but minimal awareness, easily tolerated); 2, moderate symptoms (awareness of bothersome but tolerable symptoms), and 3, severe symptoms (symptoms hard to tolerate and/or causing interference with activities of daily living, sleeping or both). The total symptom score (TSS) 4 was the sum of 4 symptom ratings ranging from 0 to 12.
Visual analogue scale
The patients expressed the global discomfort caused by AR in the previous week using a VAS. Scores ranged from 0 mm ('not at all bothersome') to 100 mm ('intolerable bothersome').
Nasal LTD4 and histamine provocation tests
Nasal LTD4 (4 to 16 mcg/mL) and histamine (0.2 to 3.2 mg/mL) challenges were performed in a stepwise manner, with the increase of nasal airway resistance (NAR) and induced symptom scores as outcomes [10]. Nasal resistance was measured with an active anterior rhinomanometry method by using a rhinomanometry (Jaeger, Würzburg, Germany) at a pressure of 150 Pa, according to the guidelines of the Standardization Committee on Objective Assessment of the Nasal Airway [11]. Nasal symptom score [sneezing <3, 0 point; 3–5, 1 point; >5, 2 point; rhinorrhea: none, 0 point; mild (<1 mL), 1 point; abundant (>1 mL), 2 point; pruritus: none, 0 point; mild (palate, eyes or throat), 1 point; severe (conjunctivitis, cough, urticaria, or difficult breathing), 2 point] were determined at 5 minutes after nasal challenge. The procedures were terminated in case of ≥60% increase in NAR or a composite symptom score being greater than 3, or until the final LTD4 or histamine diluents have been administered. Subjects with negative test results were artificially assigned 17.00 × 10-3 mg/mL for PC60NAR-LTD4 and 3.2 mg/mL for PC60NAR-Histamine.
Data analyses
Statistical analysis was performed using SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA). Qualitative data were expressed in percentages and frequencies, and quantitative data with normal distribution were expressed as mean ± standard deviation or otherwise median (interquartile range). Spearman rank test was run to determine the correlations between nasal responses to LTD4/histamine challenge and QoL. A p-value of less than 0.05 was considered as statistically significant.
RESULTS
Patient characteristics
A total of 86 patients for screening, 25 eligible patients finished both LTD4 and histamine nasal challenge and completed the questionnaire of RQoLQ, and the data were applied for analysis in this study.
The majority of patients (18 of 25) were not treated regularly prior to the study, and among them, 38.9% (7 of 18) of the patients have never been treated. 60% of AR patients were concomitant with allergic conjunctivitis, and sensitized to 2 or more allergens by SPT (Dermatophagoides [80%] was the most common allergen). The results are shown in Table 1.
Nasal responses to LTD4 and histamine nasal provocation test
The distribution of PC60NAR-LTD4 and PC60NAR-Histamine is shown in Fig. 1. PC60NAR-LTD4 varied from 1.2 × 10-3 mg/mL to 14.8 × 10-3 mg/mL, while PC60NAR-Histamine ranged from 0.3 mg/mL to 2.8 mg/mL. The potency of LTD4 in increasing nasal resistance was 142 times higher than that of histamine (PC60NAR-LTD4 9.2 (11.6) × 10-3 mg/mL vs. PC60NAR-Histamine 1.3 (2.8) mg/mL, p < 0.001).
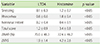
Nasal symptom score induced by histamine nasal challenge was significantly higher than that of LTD4 (3.4 ± 0.8 vs. 1.2 ± 0.9, p < 0.05). The increases of VAS were also higher after histamine nasal challenges (4.2 ± 2.6 vs. 1.9 ± 1.4, p < 0.05) (Table 2).
Scores of RQoLQ and TSS 4
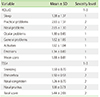
AR impaired all of the seven dimensions of health profiles of RQoLQ, especially practical and nasal problems. Symptom severity scores of the four typical AR nasal symptoms and the total score are moderately impacted by symptom severity (Table 3).
Correlations between nasal responses to LTD4 and histamine nasal provocation, TSS4 and QoL
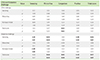
Nasal symptom scores (especially sneeze) and increased nasal resistance (ΔNAR) induced by histamine challenge were better correlated with the scores of RQoLQ than that of LTD4. The increase of nasal resistance induced by histamine nasal challenge negatively (r = –0.53, p = 0.02) correlated with the score of sleep in the AR patients. The score of sleep item was well correlated with the scores of the other 6 dimensions of health profiles in RQoLQ. Histamine nasal challenge induced sneezing, increased nasal resistant were correlated with most of the dimensions (general, practical, nasal, eye problems, and quality of sleep), while LTD4 nasal challenge induced sneeze, increased nasal resistant only correlated with nasal and ocular problems. On the contrary, the severity of the sneeze was not correlated with QoL, while the severity of rhinorrhea, congestion, and nasal pruritus were correlated with nasal and practical problems, and nasal congestion was correlated with ocular problems assessed by TSS4. The correlations of nasal responses to LTD4/histamine nasal provocation and TSS4 with QoL are presented in Table 4.
Most of histamine nasal provocation induced nasal symptoms were correlated with nasal symptom severity assessed by TSS4, while LTD4 nasal challenge induced TSS was correlated congestion in TSS4 (Table 5).
DISCUSSION
In this study, we evaluated the correlations of nasal LTD4 and histamine challenge induced nasal symptoms and nasal symptom severity (TSS4) in the previous week with QoL assessed by RQoLQ. We found that both LTD4 and histamine nasal challenge induced nasal symptom scores were mildly or moderately correlated with the overall of QoL, however, there are also differences in different dimensions of health profiles in RQoLQ. Histamine nasal challenge induced sneeze was well correlated with the dimensions of non-hay fever, practical, and nasal problems while LTD4 induced sneeze was only correlated with ocular problems in RQoLQ. Histamine nasal challenge induced increase of nasal resistance was negatively correlated with the sleep, and ocular problems while LTD4 induced increase of nasal resistance was correlated with nasal problems. This might be because that histamine nasal challenge induced typical symptoms, like sneezing and rhinorrhea, while LTD4 mainly caused longer lasting increase of NAR [12]. LTD4 and histamine may play different roles in the pathogenetic of AR. Miadonna et al. [13] and Howarth [14] have also demonstrated that the symptoms of AR such as nasal secretion, nasal obstruction, were better correlated with the release of arachidonic acid metabolites than histamine in the nasal secretion or specimen during natural exposure, but when stimulated with histamine or cysLT there was a different result, sneezing, itching, rhinorrhea, and nasal obstruction could be induced by histamine rapidly (within a few seconds), while LTs caused a more pronounced nasal obstruction. LTD4 and histamine nasal challenge tests may distinguish different phenotypes and guide the treatment of AR.
As previously reported our results also showed that nasal symptom severity (nasal congestion, rhinorrhea, and nasal pruritus) in the previous week has an impact on QoL, especially on the dimensions of practical, nasal, and ocular problems in RQoLQ [15]. Although there are some differences of the effects on QoL between the objective (LTD4 and histamine nasal challenge induced symptoms) and subjective (nasal symptom severity TSS4 in the previous week) evaluations of nasal symptoms, but, when combined LTD4 nasal challenge induced symptoms with that of histamine, the effects of nasal symptoms on QoL were consistent between objective and subjective evaluation methods. It means that LTD4 and histamine nasal challenge could distinguish which was the main inflammatory mediator under the nasal symptoms (TSS4).
Different inflammatory mediators may cause different symptoms; similar symptoms may vary in their effect on different individuals, and unlike many other disorders whose treatment may be centered on preventing death or future morbidity, the goal of treatment of AR is to improve a patient's well-being, or QoL [4]. To assess the correlation of daily AR symptom severity and nasal hyperreactivity with QoL, de Graaf-in 't Veld et al. [5] assessed 48 adults with PAR. They reported that scores for the overall and individual QoL domains of the RQoLQ were moderately but statistically significantly correlated with total nasal symptoms, with the degree of HRQoL impairment increasing with the degree of symptoms, and nasal hyperreactivity scores were significantly correlated with total and individual symptoms and overall HRQoL and individual domains except sleep and emotions. Our results suggest that combined nasal LTD4/histamine challenge with TSS4 we can individually evaluate the impacts of nasal symptoms on QoL, and identify the mainly inflammatory mediators under the symptoms.
In this study, among the 7 dimensions of health profiles, the quality of sleep was well correlated with the other 6 dimensions in RQoLQ, especially with the scores of activation, nonhyfever symptoms and emotion. As a common symptom of nasal pathology, nasal obstruction enjoys an increasing amount of interest from clinicians. Not without reason, as nasal obstruction is shown to correlate with a decreased QoL and may lead to sequel such as decreased sleep quality, rhinosinusitis, otitis media, and asthma [16]. Multitude of causes can give rise to a subjective sensation or objective presence of nasal airway restriction [17], and there are different diagnostic tools and methods for the evaluation of nasal congestion [18]. The use of tools like visual analogue scale (VAS) can subjectively reflect the severity of and affects caused by the diseases [18], while nasal LTD4 and histamine challenge with rhinomanometry can objectively evaluate nasal resistance. In our study, histamine nasal challenge induced increase of VAS was much higher than that of minimal important difference of VAS which was associated with a clinically relevant change in QoL [19]. Nasal challenge induced symptoms can be both objectively and subjectively evaluated to diminish the bias. LTD4 nasal challenge induced sneeze was also correlated with eye problems in RQoLQ. This might be because that most of the AR patients in this study were concomitant with conjunctivitis. Pathways of communication are thought to increase the likelihood of an inflammatory reaction at both sites following allergen exposure of nasal or ocular tissue [20]. AR affects the exacerbation and control of conjunctivitis, and on the opposite, the concomitant (conjunctivitis) may further impair RQoLQ [21].
There are some limitations in this study. First, the sample size did not allow for subgroup analysis using the Allergic Rhinitis and its Impact on Asthma classification. Second, the correlations between LTD4 or histamine induced nasal symptoms and the efficacy of antileukotriene or antihistamine agents need to be verified.
The present study is the first to assess the correlations of LTD4 and histamine induced nasal symptoms with QoL and TSS4. Symptoms of AR can markedly interfere with HRQoL, combined nasal challenge (with LTD4, histamine, allergens, et al.) induced nasal responses with RQoLQ can be a good diagnosis and evaluation method to guide the management of AR and help to greatly benefit patients affected by AR.



 XML Download
XML Download