

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
IgE-mediated cow's milk allergy (CMA) is one of the most common food allergies in infants and children. Its estimated prevalence is 1.9%–4.9% [1]. CMA is thought to run its course in most patients within the first year of life [2]. In Japan, the most of neonates stay in maternity hospitals for one week after birth. Some neonates were given cow's milk formula (CMF) in maternity hospitals then discontinued CMF after discharge. We often recognize that some of them develop CMA with introduction of baby food containing cow's milk protein (CMP).
A prospective population-based birth cohort demonstrated that exclusive breast feeding is associated with reduced risk of CMP sensitization [3]. Some systematic reviews showed that high-risk infants who were exclusively breast fed for at least 4 months had a lower risk of CMA than those who received CMF [4567]. Furthermore, the enquiring about tolerance (EAT) study showed that early introduction of milk dose not have any significant effects on developing CMA [8]. In contrast, the previous study showed that the early introduction of CMF reduced the frequency of CMA [9]. Although this study focused on the relationship of early introduction of CMF and development of CMA, the duration and frequency of CMF ingestion were not evaluated. Therefore, we aimed to evaluate the duration and frequency of CMF ingestion as compere with exclusive breast fed for preventing CMA in high-risk infants.
MATERIALS AND METHODS
We enrolled the patients diagnosed with hen's egg allergy by an oral food challenge (OFC) at the Aichi Children's Health and Medical Center (ACHMC) at ≤6 years of age from March 2012 to August 2015. The baseline characteristics of the subjects, perinatal information, coexisting chronic disease, atopic dermatitis in infancy, bronchial asthma before 2 years of age, family history of allergic diseases and information related to the diagnosis of CMA were obtained from the patients' medical records. These variables were adjusted for statistical analyses.
A questionnaire was completed by the caregivers of patients from September to December 2015 regarding the timing of the introduction and discontinuation of CMF (within the first week of life, from the first week to 1 month, and from 1 to 3 months), and the frequency of CMF ingestion (at least once daily, 2–4 days per week, ≤1 day per week). We did not account hydrolyzed formulas as CMF, and no participants were fed amino acid formula. We also checked the subjects' feeding status in infancy from the initial medical record and the maternal and child health handbook to reduce the recall bias and misclassification.
The diagnostic criteria of CMA for patients was to have both following conditions; (1) a positive OFC result or any convincing episode of immediate reaction within 2 hours after the ingestion of a cow's milk product and (2) positive cow's milk-specific IgE (CM-sIgE, >0.34 KUA/L). The concentration of specific IgE antibody was measured from sera using ImmunoCAP system (Thermo Fisher Diagnostics, Tokyo, Japan).
Based on the information, we analyzed the relationship between the duration and frequency of CMF ingestion in the first 3 months of life and the development of CMA at 3–24 months of age. We also evaluated the maximum CM-sIgE titer and the achievement of tolerance at <72 months of age. In this research, we regarded patients as who achieved tolerance according to the capability of quantity cow's milk ingestion (100 mL/dose for <36 months of age, 200 mL/dose for ≥36 months of age) with no symptoms.
All statistical analyses were performed using the EZR software program (Saitama Medical Center, Jichi Medical University, Saitama, Japan) [10]. This retrospective data analysis was approved by the institutional ethical committee of ACHMC.
RESULTS
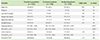
Three hundred ninety-seven of the 520 potential eligible patients (positive egg OFC) came to the hospital for a follow-up examination within the study period (Fig. 1). Twenty-three of the 397 patients were excluded for the following reasons: incomplete questionnaires (n = 11), underlying diseases (n = 2), developing CMP-induced enterocolitis syndrome (n = 1), and developing CMA before 3 months of age (n = 9). No significant difference was observed in the baseline characteristics of the excluded patients and the analyzed patients except the maximum total IgE and egg white-specific IgE titers (Table 1).
The analyzed patients were categorized into the following subgroups: exclusively breast fed (breast-fed group, n = 75); discontinued ingestion of CMF before 3 months of age (temporary group, n = 177); continuous ingestion of CMF, but not daily, up to 3 months of age (nondaily group, n = 47); continuous ingestion of CMF at least once daily (daily group, n = 75) (Fig. 1). One hundred seventy-one patients (45.7%) were diagnosed as CMA after 3 months of age.
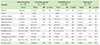
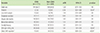
The incidence of developing CMA between the breast-fed group and temporary group did not show any statistical difference. However, nondaily group and daily group had a significantly lower incidence of developing CMA in comparison to the Breast-fed group (nondaily group odds ratio, 0.43; p = 0.02; daily group odds ratio, 0.11; p < 0.001) (Table 2). In the multivariate logistic regression analysis, the ingestion of CMF at least once daily until the first 3 months of age was independently associated with the lower incidence of developing CMA (adjusted odds ratio, 0.16; p < 0.001) (Table 3). However, we did not detect obvious relationship between CMF ingestion and the maximum CM-sIgE titer or the achievement of tolerance (Table 2).
DISCUSSION
The recent publication of randomized trials suggested that early oral exposure to food antigen induces tolerance [811]. The learning early about peanut allergy study showed that a lower ratio of peanut-specific IgG4:IgE was associated with peanut allergy [11]. In our study, the daily group had a significantly lower incidence of developing CMA in comparison to the breast-fed group whereas the incidence of developing CMA in the temporary group did not have statistical difference. Additional prospective cohorts should be needed to evaluate the elevation and transplacental transport of cow's milk specific IgG4. EAT study performed early-introduction of multiple allergenic foods including CMP from 3 months of age in an unselected population of exclusively breastfed infants. Furthermore, the ingestion of CMP was nondaily. As a result, no significant effect of early-introduction of CMP to prevent CMA was demonstrated [8].
In our study, we selected the patients with confirmed hen's egg allergy as a high-risk group and evaluated the development of comorbid CMA. The relatively high CMA comorbidity (45.7%) in the subjects was due to the highly specialized role of our institute where complicated cases tend to be consulted from the local pediatricians. The result demonstrated that high-risk infants who ingested CMF daily up to 3 months of age showed lower frequency of developing CMA compared to the high-risk infants with exclusive breast feeding. Although a similar finding has previously been reported [9], this is the first report to suggest the duration and frequency-dependent effect of CMF ingestion in the prevention of CMA.
Eleven patients of the daily group (14.7%) developed CMA. Most of them were predominantly breast-fed and added small amount of CMF. Some of them had allergic reaction when they intake a large amount of CMP such as cheese for the first time (data not shown). This suggests that the amount of CMF ingestion might also be considered to evaluate the effect and risk of early ingestion of CMF.
Traditionally, it was thought that CMA was resolved by 1 to 2 years of age. However, Carroccio et al. [12] found the proportions of Italian infants with CMA who achieved tolerance at 1, 2, and 3 years after initiation of milk-free diets were 30%, 54%, and 70%, respectively. Vanto et al. [13] also showed the proportions of Finnish infants with CMA who achieved tolerance at 2, 3, and 4 years of age were 31%, 53%, and 63%, respectively. The rates of persistent CMA in our study (49.1% at 5 years of age) were similar to these findings. When comparing the prevalence of persistent CMA between the groups, there were no significant differences. From this result, early introduction of CMF may affect the onset of CMA while the achievement of tolerance may be associated by re-introduction of CMP after diagnosis of CMA.
The temporary group included nine patients who changed CMF to hydrolyzed formula before 3 months of age. The reasons of starting hydrolyzed formula were the instruction by their maternity hospital (n = 4), diarrhea (n = 1), eczema (n = 2), and eczema with positive CM-sIgE (n = 2). Three of the last 4 patients with eczema developed CMA afterward.
Katz et al. [14] demonstrated that the cumulative incidence for CMP-induced enterocolitis syndrome was 0.34% in a large-scale, population-based prospective study. In our study, one of the patients developed CMP-induced enterocolitis syndrome (0.2%), yet no patient was diagnosed as cow's milk intolerance.
The limitation of our study was due to its retrospective style. The possibility of reverse causation was minimized by excluding the cases which developed CMA before the age of 3 months. Although we checked the feeding records in the initial medical record and a patients' maternal and child health handbook, a recall bias regarding to the feeding status in infancy might be inevitable. Another limitation is the highly selected subjects (confirmed egg allergy as high-risk infants), so the result cannot be generalized to the normal populations.
The advantage of breast feeding in providing essential nutrients and immunomodulatory effects has been noted in many studies. In this research, most of the patients with CMF ingestion started with mixed feeding, and discontinued CMF afterward. So, the result does not deny the advantage of breast feeding. Additional prospective cohorts should be needed to confirm this observation.

 XML Download
XML Download