

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Atopic dermatitis (AD) is one of the most prevalent inflammatory skin disorders affecting infants and young children [1, 2]. As a chronic disorder with increasing prevalence worldwide, AD imposes substantial economic and quality of life (QoL) burden on patients, families, and societies [3, 4, 5, 6, 7]. Studies in the Asia-Pacific region show that the annual direct AD cost alone (expressed in 2013 United States dollars [US $]) ranges from US $199 in Thailand [8], to US $1,253 in South Korea [9], and to US $4,842 in Australia [6].
A combination of genetic, immunologic, and environmental factors affect AD incidence risk. In particular, exposure within the first 6 months of life to dietary allergens such as proteins found in standard cow's milk formula (CMF) can increase this risk. Such exposure can be particularly problematic among high-risk infants with atopic heredity (e.g., those having 1 or more parent or sibling with a history of allergic disease/first degree atopic heredity [10, 11, 12]). As a result, the standing World Health Organization (WHO) recommendation of exclusive breastfeeding through the first 6 months of life [13, 14, 15] may apply particularly in this high risk population. However, in some cases following these recommendations is impossible and infant formulas are used as nutritional supplement to or replacement for breast milk. In such instances, partially hydrolyzed formulas (PHF) or extensively hydrolyzed formulas (EHF) containing whey (W) and/or casein (C) as a protein source [16, 17] may be used as an alternative to CMF as hydrolyzed infant formulas may reduce the risk of AD and other allergies [10, 18, 19]. In particular, results from the German Infant Nutritional Intervention (GINI) study, the largest trial comparing the impact of a 17-week early nutritional intervention with PHF-W vs. CMF among nonexclusively breastfed infants with atopic heredity, showed a lower 6-year cumulative AD incidence with PHF-W relative to CMF (adjusted relative risk [RR], 0.64; 95% confidence interval [CI], 0.48-0.86) [10]. In addition, results from a randomized trial of genetically predisposed Singaporean infants found that the cumulative AD incidence at 24 months of age was 22.6% with PHF-W and 43.9% with CMF [20]. These results, confirmed via meta-analyses [19, 21], have led national and international allergy organizations to suggest the use of hydrolyzed formulas as an allergy risk-reduction strategy for formula-fed high-risk infants who are not exclusively breastfed [12, 22, 23, 24].
AD risk reduction with PHF-W in high-risk infants may result in clinical, economic, and QoL benefits. These benefits however, must be weighed against the potentially higher costs of PHF-W relative to CMF during the 17-week interventional period. Several economic studies conducted in developed countries suggest that PHF-W is cost-effective, if not cost saving, versus CMF in high-risk infants not exclusively breastfed [25, 26, 27, 28, 29, 30, 31]. However, a search of the literature indicates that comparable evidence is extremely limited for developing nations. A study has recently reported that PHF-W is cost effective vs. CMF in the Philippines [31], saving US $237 per infant.
Relying upon health economic modeling techniques to aggregate data from multiple sources, including the GINI study [10] and expert opinion, this study was conducted to estimate the longterm (i.e., birth to 6 years of life) clinical and economic impact of feeding with PHF-W versus CMF for the first 17 weeks of life on AD risk reduction among high-risk infants in urban Malaysia.
MATERIALS AND METHODS
Model overview and key assumptions
Markov cohort modeling techniques [32, 33] were used to compare costs and outcomes in the first 6 years of life associated with AD risk reduction using PHF-W (here assumed to be NAN HA, Nestlé (M) Sdn Bhd, Petaling Jaya, Selangor, Malaysia) vs. CMF (here assumed to be Enfalac A+, Mead Johnson Nutrition (M) Sdn Bhd, Petaling Jaya, Selangor, Malaysia) in the first 17 weeks of life among healthy (i.e., without a previous AD diagnosis), nonexclusively breastfed, high-risk (with first degree atopic heredity) infants in urban areas of Malaysia. The target population, risk reduction, formula feeding and duration, and AD incidence were based on the GINI study [10, 18].
The model incorporated direct and indirect costs associated with AD treatment and formula feeding from the perspective of urban populations. The analytical horizon (i.e., from birth to 6 years), consistent with the GINI study, was used to capture longer term effects [10]. The primary outcomes for each treatment arm included cost (overall and differences), AD incidence, number of days without AD flare, time spent post-AD diagnosis, and QALYs.
A simplified diagram of the model structure is presented in Fig. 1. Infant cohorts entered the model at birth and were followed in bi-weekly cycles until 6 years of age. Infants continued to be fed with the initially assigned formula (PHF-W or CMF) until week 17, unless AD developed. As in the GINI study, AD incidence varied by age and initial formula used (PHF-W or CMF). Similar to previously-published models [25, 26, 27, 29, 30, 31], up to 3 treatment approaches were considered upon AD development: formula switch only, pharmacotherapy only, and combination formula switch and pharmacotherapy. These approaches were endorsed by Malaysian pediatricians with experience treating pediatric AD patients (authors AHAL, SW, PCK). If a child responded to a formula switch, they were assumed to continue on that formula until up to 12 months of age, the next AD episode, or death, which, for simplicity, was not depicted as a separate state in Fig. 1 but was included in the model. In case a child did not respond to a formula switch, she/he was assumed to be switched to another formula. The first switch formula was assumed to be soy, followed by PHF-W for those who were initially on CMF and EHF for those who were initially on PHF-W. A child who responded to pharmacotherapy was assumed to complete the treatment course and remain on their formula until up to 12 months of age. Infant formula use was assumed to end at 12 months of age; hence, the pharmacotherapy only treatment approach was always used from year 1 to year 6.
Treatment success (i.e., response to treatment approach) was defined as complete AD symptom resolution and was assessed every 2 weeks. Assumptions regarding response rates determined the speed at which children experienced AD symptom resolution and transitioned to an AD-controlled state (ADCS). Response rates varied according to AD severity, treatment approach, and line of treatment. Following remission into ADCS, a child could experience a flare, the rate of which was dependent upon age group (0-1 years; >1-6 years) and AD severity (mild, moderate, and severe).
A lack of uniformity exists in methods to determine AD disease severity internationally [34]. The various available scales are rarely used in clinical practice [34]. While there is no gold standard, scoring atopic dermatitis (SCORAD) is among the most commonly used validated scales, which incorporates both objective and subjective assessments [34]. Therefore, in this analysis, AD severity (mild, moderate, severe) was assumed to be based on the SCORAD index (Eczema grading: mild < 25, moderate 25-50, severe > 50) [35], especially in discussions among the Malaysian pediatricians who provided inputs for the analysis.
Clinical and epidemiologic inputs
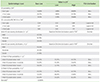
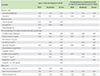
Epidemiologic inputs are listed in Table 1. The probability of AD for PHF-W and CMF was obtained using linear interpolation of the 1-, 3-, and 6-year cumulative incidence data from the GINI study [10]. The distribution of AD cases and probability of flares by severity and age group were derived from the aforementioned expert opinion. Clinical management and treatment effectiveness inputs which include rates of AD management modality and response rates were stratified by AD severity, treatment line, and age group (Table 2).
Resource use inputs
Daily formula intake was derived using a previously reported method [26] and accounted for partial breast feeding and agerelated nutrition requirements.
Table 3 details the other resources used to manage AD. Information on the type and amount of resources used with each treatment modality based on AD severity was provided by the experts. Specifically, the frequency of outpatient visits (general pediatrician or specialist, i.e., allergist, dermatologist) and inpatient visits were dependent on AD severity and treatment response. Based on the experts' opinions, hospitalizations were assumed to occur in 2 out of 1,000 subjects with severe AD less than 1 year old upon initial AD development. Whereas hospitalizations were assumed to occur in approximately 4 out of 100 severe AD patients 1-6 years of age upon initial development of AD.
Diagnostic tests were assumed to be performed in some but not all AD patients. Skin prick tests, specific IgE and oral challenge tests were assumed to be performed upon initial AD development depending on AD severity. Inpatient and outpatient visits and diagnostic tests costs were based on average fees charged in Malaysia in selected private or government hospitals or laboratories in the Kuala Lumpur Metropolitan Area where information was available.
Nearly all AD patients were assumed to be prescribed emollient and/or moisturizer creams upon initial AD development and again during reassessment consultation visits in case of nonresponse and/or flare.
Cost inputs
Table 4 provides data on cost. Formula acquisition costs were based on the market share in Malaysia (Source: Packaged Food: Euromonitor from trade sources/national statistics, February 2013) and reflected the formula cost paid "out-of-pocket" by families because infant formula is not covered by private or public insurance companies in Malaysia. Only the additional costs incurred as a result of feeding an alternative infant formula for AD prevention or treatment (such as PHF-W, soy-based formula, and EHF) as opposed to CMF were included in the analysis. Medicine acquisition costs were obtained from an online drug information tool (http://www.mims.com/Malaysia) commonly used in Malaysia. Reduced productivity (i.e., indirect costs) included lost work days to care for a child with AD following the initial physician visit (irrespective of AD severity).
Utility inputs
A utility of 1.000 was assumed for children who did not develop AD; a utility of 0.980 was assumed for children in ADCS to recognize that mild, subclinical episodes can reduce QoL. A utility of 0.863 was associated with ongoing mild, 0.690 with moderate, and 0.450 with severe AD episodes based on previously published data [36, 37]. Death was associated with a utility of 0.000.
Statistical analysis
Using the model structure and inputs detailed herein, several incremental cost effectiveness ratios (ICERs) were computed to estimate the economic value of PHF-W compared to CMF. These outcomes included the incremental costs per AD case avoided, per days without AD flare gained, and QALYs gained. In addition, AD costs per AD patient overall and per year and AD visits per AD patient per year were derived from the model to allow validation of these values with other published estimates.
Sensitivity analyses were conducted to evaluate the robustness of the results. First, deterministic univariate sensitivity analyses (uSA) varied individual model parameters while keeping other base-case values unchanged (see Tables 1, 2, 3 for ranges). Scenario analyses were conducted to test the impact of changing key model assumptions either alone or in combination. These included omitting any flares from the analysis and restricting the analysis to 1 year (as opposed to the 6-year time frame). Multivariate, probabilistic sensitivity analysis (PSA) was conducted whereby the model was run 5,000 times via Monte Carlo simulation to estimate bootstrapped 95% Bayesian CIs.
In accordance with common health economics research guidelines, clinical and economic outcomes occurring after the first year were discounted at 3% per annum to estimate the net present value of the different strategies, reflecting society's preference for the present. Costs reported in this study represent 2013 values, expressed in Malaysian Ringgit and US dollars (MYR; MYR 1,000 = US $316.50; 25-Oct-2013).
Finally, this study was exempted from the Malaysian Medical Research Ethics Committee review and approval as per its guidelines 4a.
RESULTS
Children who developed AD within the first 6 years of life were predicted to incur an undiscounted total (direct and indirect) AD cost of MYR 7,990 (US $2,529; 95% CI, MYR 6,211-9,826) on average. The cost of AD was MYR 5,245 (US $1,660) for mild cases, MYR 7,397 (US $2,341) for moderate cases, and MYR 15,060 (US $4,767) for severe cases. The estimated average annual undiscounted total (direct and indirect) cost for an infant developing AD within the first 6 years of life was MYR 1,885 (US $584; 95% CI, MYR 1,567-2151) including MYR 1,256 (US $398) in direct costs alone. The corresponding costs if all cases were assumed to be mild were MYR 1,211 (US $383), moderate MYR 1,708 (US $541), and severe MYR 3,478 (US $1,101). Finally, the total annual number of visits per AD case was estimated at 6.88 visits across all cases and 4.38 visits for mild, 7.02 for moderate, and 12.26 for severe cases.
As Table 5 shows, compared to CMF, PHF-W was associated with lower AD incidence (-14%, 39% vs. 25%; 95% CI for the difference: 3%-23%), fewer years post-AD diagnosis (-0.69 years, 1.69 years vs. 1.01 years; 95% CI for the difference: 0.25-1.10 years), and fewer AD-flare days (-38 days, 55 days vs. 93 days; 95% CI for the difference: 2-94 days). Discounted QALYs with PHF-W were 5.517 QALY (95% CI, 5.440-5.547 QALY) versus 5.479 QALY (95% CI, 5.369-5.528 QALY) with CMF, for a net difference of 0.038 QALY (95% CI, 0.016-0.079).
The total discounted costs (direct and indirect) of AD risk reduction among the nonexclusively breastfed infants with atopic heredity were lower among those fed PHF-W (MYR 1,758 [US $556]; 95% CI, MYR 917-3,033) compared to CMF (MYR 2,871 [US $909], 95% CI, MYR 1,697-4,278). Primary drivers of total costs were those associated with pharmacological treatments followed by indirect costs and physician visits.
The resulting 6-year net savings due to AD risk reduction with PHF-W was MYR 1,113 (US $352) (95% CI, MYR 317-1,884), irrespective of AD development (Table 5). After 1 year, the total discounted cost for PHF-W versus CMF was MYR 173 (US $55) versus MYR 312 (US $99). In fact, PHF-W was associated with a net cost-savings almost immediately after formula initiation.
Comparison of PHF-W versus CMF using ICER values showed PHF-W to be a net cost-saving strategy which also resulted in reductions in avoided AD cases, gains in days without AD flare, and QALY gains (i.e., PHF-W is the "dominant" strategy) relative to CMF (Table 4). Additionally, results from the PSA indicated that PHF-W was dominant (more effective and less expensive) in 99.6% of the 5,000 model runs (Fig. 2).
In uSA, the RR of developing AD between CMF and PHF-W and the absolute risk of AD with CMF had the largest influence on the difference in cost between PHF-W and CMF. Other variables with potentially minor effects on net cost savings were PHF-W, CMF, and emollient costs. Finally, PHF-W remained cost dominant resulting in a net saving of MYR 407 (US $129) and discounted gains of 0.016 QALY when it was conservatively assumed that no AD patient would experience a flare.
DISCUSSION
Based on the model presented herein, early nutritional intervention with PHF-W in healthy infants with atopic heredity who are not exclusively breastfed is cost saving and improves health relative to CMF. In the base case, PHF-W was associated with a decrease in AD risk and an increase in days without AD flare and QALYs. Accordingly, PHF-W also resulted in net statistically significant discounted cost decreases of MYR 1,113 (US $352) (95% CI, MYR 317-1,884) per infant (from MYR 2,871 [US $909] to MYR 1,758 [US $556]), after including the additional cost of PHF-W over CMF. The robustness of these results was confirmed via comprehensive sensitivity analyses.
The cost differential between the two arms considered herein was driven primarily by the following cost categories: pharmacotherapy, indirect costs, and physician visits. All other costs had minimal impact, including the formula costs for PHF-W and CMF, which were nearly similar. Pharmacotherapy costs were high because it was the most common treatment method utilized either alone or in combination with formula change. Physician visit costs were relatively expensive because of the number needed for AD management, averaging 6.92 visits per year reflecting in part the need for visits associated with frequent flare recurrence. To assess how the assumptions regarding flare recurrence impacted the results, a scenario analysis assumed no relapse. In this case, PHF-Wassociated cost-savings were reduced from MYR 1,113 (US $352) to MYR 407 (US $129).
Outcomes presented herein are consistent with similar analyses in developed countries [25, 26, 27, 30] whereby PHF-W was cost effective or cost saving (depending on whether a third party payer or societal perspective was adopted). These are also consistent with an analysis conducted in the Philippines which showed that PHF-W results in savings of US $247 (95% CI, 94-323) in a similar target population. These similarities can be partially attributed to shared methodology and assumptions [25, 26, 27, 28, 29, 30]. In contrast, the annual total (MYR 1,845 [US $584]) and direct (MYR 1,256 [US $398]) AD costs among those who developed AD were somewhat higher than in Thailand [8] (US $199 for direct cost), but lower than in South Korea [9] (total cost, US $3,522; direct cost, US $1,253 in a sample of pediatric patients from an allergy clinic) or Australia [6] (total cost, US $6,187; direct cost, US $4,842 in a sample of pediatric patients from a dermatologic clinic). Differences reflect variations in study design and methods, target patient populations, and per-capita income. Consistent with disparities reported in other studies [6, 8], annual AD costs increased with worsening disease severity, from MYR 1,211 (US $383) for mild cases to MYR 3,478 (US $1,101) among severe cases.
The annual number of physician visits necessary to manage AD (6.88 across all cases, 4.38 visits in mild, 7.02 visits in moderate, and 12.26 visits in severe cases) may be conservative when compared to values for Australia [6] (12.88 visits overall; 7.0 visits in mild, 13.0 visits in moderate, and 23.2 visits in severe cases) but very consistent with Thailand [8] (approximately 4.3 to 4.6 visits overall; 4.0 visits in mild, 8.0 visits in moderate, and 12 to 13 visits for severe cases)
This analysis was limited by a lack of published data specific to Malaysia regarding AD epidemiology and treatment patterns and the impact of PHF-W and CMF on AD incidence. Consequently, we relied on the GINI trial results [10] and the clinical opinion of 3 physicians in Malaysia experienced in treating pediatric AD patients. This challenge is not unique to Malaysia. In both developed and developing countries, AD is diagnosed clinically and severity is assessed subjectively. It is not routinely recorded administratively (e.g., for reimbursement). Hence, in many nonprospective studies, AD severity cannot be asserted definitely. Many AD treatments (e.g., formula replacement or over-the-counter topical agents) require out-of-pocket expenditure borne by families. These may be under-recorded and are difficult to estimate. As a result, even analyses conducted in developed countries [25, 26, 27, 28, 29, 30] relied heavily on similar evidence and input generation methods reported herein.
Exclusive reliance on GINI trial data as the efficacy source for different infant formulas in this analysis was justified on the grounds that it is the largest randomized, double-blind, interventional trial with the longest follow-up period comparing PHF-W and CMF [19, 21]. In addition, the cumulative AD incidence rates observed in GINI for PHF-W and CMF are consistent with and perhaps conservative compared to those observed in a smaller study by Chan et al. [20], 2002 (n = 110) in hereditarily predisposed Singaporean infants. Specifically, cumulative AD incidence in the CMF arm was 43.9% and in the PHF-W arm 22.6% at 24 months of age in the Singaporean study (odds ratio, 0.37; p = 0.019) [20]. Conversely, corresponding unadjusted rates in the GINI trial were 33.5% and 39.1% in the CMF arm and 19.5% and 27.4% in the PHF-W arm after 3 (adjusted RR, 0.58; 95% CI, 0.41-0.82) and 6 years (adjusted RR, 0.64; 95% CI, 0.48-0.86) respectively [10]. These relatively high rates of AD are also in line with a 39.3% prevalence of eczema observed among Malaysian adolescents (age 11-20 years) with a family history of asthma and allergy [38].
Little evidence is available regarding AD severity in Malaysia and elsewhere. In the present analysis, AD severity was assumed to be moderate in 37% of cases in children less than 1 year of age and in 28% of cases in children aged 1 to 6 years; AD was assumed to be severe in 20% of cases in children aged less than 1 year and in 22% of cases in children aged 1 to 6 years. In the International Study of Asthma and Allergies in Childhood [39], severe AD (defined as current eczema associated with sleep disturbance 1 or more nights per week) accounted for 7% of AD cases in those aged 6 to 7 years old. Results from a survey of Southeast Asian dermatologists assessing knowledge, attitudes, and practices on AD management [40], found that 14% of patients initially presented with severe, 18% with mild, and 68% with moderate disease. Thus, the assumptions used herein may be considered reasonable given that the population considered was high-risk infants (≥1 parent or sibling with history of allergic disease/first degree atopic heredity). At the same time, it should be noted that the assumptions regarding both the severity and prevalence of AD adopted herein were meant to be applicable to an urban population. Thus, the outcomes of this analysis could have been dramatically different had we adopted a rural or government practice perspective.
Treatment and resource use patterns for AD are poorly documented in Malaysia. A literature search identified one survey of 44 dermatologists regarding AD management treatment patterns in Malaysia [40]. Moisturizers were reported to be always used by 77% of respondents in the clearance phase of treatment and in 86% of patients in the maintenance phase of treatment. Participants reported prescribing topical steroids for approximately 34% of infants with mild, 57% with moderate, and 9% with severe AD. Low potency topical corticosteroids were used most frequently (93%) in infants and children. Eighty percent reported 'always' prescribing oral antihistamines to treat AD patients. In severe AD, oral steroids were used by 93% of dermatologists. Phototherapy was reportedly used by 25% of dermatologists. Finally, 5% recommended the use of alternative medicines such as traditional Chinese medicines and homeopathy. These treatment patterns-while different than assumed herein in part perhaps because the survey respondents were dermatologists whereas the present analysis adopts a primary care view point-indicate that the management of AD in Malaysia may be relatively intense. In the present analysis, it was assumed that a high proportion of patients would receive topical therapy (with moisturizers and/or topical steroids). On the other hand, the use of oral steroids and phototherapy was not considered.
Food allergens, especially cow's milk, are often implicated as major triggers for AD relapse/flare-ups in infants. Whether confirmed by diagnostic testing or suspected by clinical history, shifting to a non-CMF is common practice. Here, the use of soy-based formulas was selected as a method to manage AD triggered by a cow's milk allergy to reflect current practice in Malaysia, after taking into account the lower cost and superior palatability of soy formula relative to other formulas. However, soy-based formulas, as a rule, are not recommended for AD treatment unless a substitute formula is necessary for cow's milk-allergic children with moderate to severe AD who cannot afford the cost of EHF. In part, this assumption could be considered conservative because the use of the least expensive dietary modification available in Malaysia (i.e., soy formula) may underestimate AD management costs and subsequently the value of preventing and/or reducing AD. This study did not account for any wastage factor while estimating costs for formula consumption; although, varying formula acquisition costs in sensitivity analysis indicated by proxy that this consideration has a limited impact on outcomes.
This study was conservative in additional aspects. First, any effects of AD beyond the first 6 years of life were excluded. In addition, any other allergic manifestations (within and after the initial 6 years) that may be preventable via PHF-W were also ignored. The impact of AD on parents' productivity and, in particular, lost productivity while at work as a result of a poor night sleep to attend to a crying child, etc. was only partially considered, in part due to a lack of data. The impact of AD on parents' QoL was ignored entirely.
In conclusion, exclusive breastfeeding is recommended by the WHO for the first 6 months of life. The present analysis modeled the long-term cost-effectiveness of AD risk reduction via early nutritional intervention with PHF-W versus CMF in healthy Malaysian urban infants with atopic heredity (high-risk) who are not exclusively breastfed. The results suggest that PHF-W used in this population may be a dominant strategy compared to CMF as it reduces the clinical and QoL burden of AD while decreasing overall costs, even after including formula costs. The results provide valuable insights into the long-term risk reduction of AD in children that can be helpful for physicians. Furthermore, it may help private health insurance planners make decisions regarding reimbursement/coverage policies for infant formulas among infants who are predisposed to developing AD and who are not exclusively breastfed. While the analysis was conducted on the basis of limited evidence, various sensitivity and scenario analyses show that these conclusions may be robust. Nevertheless, additional research regarding the epidemiology, severity, treatment patterns, and resource use associated with the risk reduction and treatment of AD in Malaysia are warranted.





 XML Download
XML Download