

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Allergic rhinitis (AR) is a common disorder with an estimated prevalence of 10-20% in the United States and Europe [1]. It is also one of the most common reasons for consultation in general practice clinics [2]. In the Philippines, the prevalence among adults is estimated to be 20% [3]. The Allergic Rhinitis and Its Impact on Asthma (ARIA), published in 2001 and recently updated in 2010, is designed to standardize diagnosis and management of AR [4]. Knowledge and treatment of AR by physicians consistent with consensus guidelines is reported to result in significantly better patient outcomes [5]. However, not all physicians who treat AR may be aware of or follow recommendations contained in guidelines. A survey of specialist physicians in Belgium shows that 90% of their otolaryngologist respondents have heard of ARIA. Of those who are aware of the guidelines, 62% report that they always or mostly follow the ARIA algorithm in their daily management [6]. A study of Italian general practitioners (GPs) shows that they treat patients independently of guidelines [7]. In Southeast Asia, a survey of Malaysian ENT (ear, nose, throat) specialists and GPs shows that their management of mild and moderate to severe AR is consistent with ARIA guidelines [8]. Other studies describe physician perspectives on disease burden and AR management [9101112]. However, compared to other regions of the world, Asian data on physician attitudes and practices on AR is limited. This study partially addresses this gap by assessing awareness of and adherence to guideline recommendations on the diagnosis and management of AR among specialist and general physicians in the Philippines.
MATERIALS AND METHODS
Respondents
This study was approved by the Institutional Scientific and Ethical Review Boards of St. Luke's Medical Center. A cross section of specialist and general physicians practicing in the National Capital Region (NCR) of the Philippines were surveyed from November 2014 to January 2015. General physicians were defined as family physicians and internal medicine physicians without subspecialty training while specialist physicians were otolaryngologists and internal medicine physicians with specialty training in pulmonology or allergology. Respondents were identified from a merged database of component medical societies (Philippine Academy of Family Physicians and Philippine College of Physicians) of the NCR for general physicians and from subspecialty societies (Philippine Society of Otolaryngology-Head and Neck Surgery, Philippine College of Chest Physicians, and Philippine Society of Allergy, Asthma and Immunology) for specialist physicians.
Physicians were included in the study if they had been practicing for a minimum of 5 years with adults comprising at least 60% of their total patient population. Excluded were physicians employed by pharmaceutical companies and those who were investigators in clinical trials involving medications or interventions for AR.
Questionnaire
A questionnaire, modeled after previously published surveys, was designed for this study. The questionnaire was divided into three domains to address awareness, attitudes and practices. Questions under the awareness domain were designed to assess knowledge of the existence of guidelines for the diagnosis and treatment of AR. Questions under the attitudes domain were designed to assess basis for AR diagnosis and management. For respondents who reported awareness of the existence of guidelines, additional questions assessed adherence to guideline recommendations and attendance in continuing medical education (CME) activities. For the domain on practices, questions were designed to elicit most commonly used diagnostic tests, preferred first and second line treatment, duration of treatment and preferred alternative treatments. The questionnaire was validated and pilot tested for clarity as a survey tool.
Data collection, encoding, analysis
The target sample size was 100 for general physicians and 100 for specialist physicians for a margin of error of 9.8%. The specialist physicians sampled were subdivided into otolaryngologists, pulmonary medicine physicians, and allergologists based on the proportion of each groups' number in the NCR compared to their total number in the entire country. Sample size was based on budgetary constraints (i.e., the cost for a third party research agency to conduct the field surveys).
The NCR was divided into north, south, west, and east sectors. A total of 100 specialist (25 respondents/sector) and 100 general physicians (25 respondents/sector) were selected using systematic randomization. Sampling began with a random start and subsequently every kth element on the database was selected using a sampling interval. In case of nonavailability after two call backs or refusal to participate in the interview, another substitute physician from the same area was chosen, subject to the same randomization method, until the predetermined number of respondents was reached. The face to face structured interviews were conducted by experienced interviewers from the research agency PREMIS (Philippine Research and Marketing Information Services). To ensure accuracy of data collection, 20% of the interviews were spot checked and back checked, 10% were directly observed and all survey results were assessed for completion and consistency of data. Data was encoded on MRDCL (http://www.mrdcsoftware.com/products/mrdcl).
The answers for each question in the survey were reported as a percentage of the total physician responses for specialists and generalists. Z test was used to test for significant differences between the two groups. Level of significance was set at p < 0.05.
RESULTS
To reach the predetermined sample size, a total of 555 general physicians and 634 specialist physicians were randomly selected and invited to participate in the survey. Of the generalist respondents, 56% were GPs or family physicians and 44% were internal medicine physicians. For the specialist respondents, 54% were otolaryngologists, 44% were pulmonary medicine physicians, and 2% were allergologists. The profiles of each group are summarized in Table 1. General physicians saw a median 150 patients/wk while specialist physicians saw a median 60 patients/wk. For the number of AR patients seen/wk, general physicians saw 1 in 10 versus specialist physicians who saw 1 in 3. When given the ARIA definitions of mild and moderate-severe AR, both groups reported treating the same number of patients with mild AR (10/wk). However, specialists treated twice the number of patients with moderate-severe AR compared to generalists (10/wk vs. 5/wk) and the difference was significant (p < 0.05). Asthma (71% of generalists, 75% of specialists) followed by sinusitis (6% of generalists, 15% of specialists) were the most common comorbid conditions seen in AR patients.
Awareness
Fifty-four percent of generalists versus 84% percent of specialists reported adherence to guidelines on AR; the difference was significant (p < 0.05). When asked which guidelines they followed, 74% of general physicians and 90% of specialist physicians cited ARIA. More generalists compared to specialists reported adherence to guidelines other than ARIA (26% vs. 10%, respectively). Among the respondents who reported adherence to guidelines, 59% of generalists and 37% of specialists were aware of ARIA but could not recall its meaning. Fifteen percent of generalists and 54% of specialists were aware of and knew the meaning of ARIA. The differences were all significant (p < 0.05).
There was also a significant difference between self-assessed adequate knowledge about AR between generalists and specialists (39% vs. 58%, respectively). Both groups felt that CME activities on AR were helpful and applicable to their practice (65% of generalists, 67% of specialists). Both groups cited local triggers of AR as the topic that needed further study. Both groups (73% of generalists, 88% of specialists) felt that most patients were not knowledgeable about AR and there was a need to educate them. Economic reasons were cited by both groups as their perceived reason for patients' noncompliance with AR treatment (93% of generalists, 76% of specialists).
Attitudes and practices
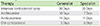
General and specialist physicians did not routinely use diagnostic tests (92% and 81%, respectively). Among the physicians who reported treating patients with mild AR, monotherapy was the preferred first line of treatment (82% of generalists, 77% of specialists). Both groups preferred antihistamines for monotherapy (Fig. 1). The most common reasons cited for antihistamine use as first line of therapy were efficacy (74% of generalists, 63% of specialists), "recommended by guidelines" (18% of generalists, 30% of specialists) and affordability (14% of generalists, 21% of specialists). Both groups reported one week as the preferred duration of antihistamine use. The preferred duration of use for other drugs are summarized in Table 2. Across the various therapeutic classes of drugs for mild AR, both groups tended to name branded drugs rather than generic drugs when asked about their most commonly prescribed medicine.
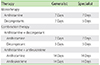
Preference for monotherapy versus combination therapy for the management of moderate-severe AR was similar for both groups (44% vs. 56% for generalists and 49% vs. 51% for specialists). Both groups preferred intranasal corticosteroid spray (INCS) for monotherapy (Fig. 2). The most common reasons cited for INCS use as monotherapy were efficacy (92% of generalists, 67% of specialists) and "recommended by guidelines" (12% of generalists, 31% of specialists). One month was the preferred duration of use for INCS as monotherapy. Both groups preferred antileukotrienes, antihistamines and INCS for combination therapy (Fig. 2). Both groups similarly prescribed combination therapy for a duration of 1-2 weeks. The preferred duration of use for other drugs is summarized in Table 3. As with mild AR, both groups tended to name branded drugs rather than generic drugs when asked about their most commonly prescribed medicine for moderate-severe AR.
For adjuvant therapy, general physicians (82%) preferred vitamins; nasal irrigation/douche was preferred by specialists (82%).
DISCUSSION
The NCR has the greatest concentration of physicians in the Philippines. Fifty-five percent (5,000/9,000) of general internal medicine physicians, 26% (1,323/5,019) of family physicians, 60% (600/1,000) of pulmonologists, 46% (307/661) of otolaryngologists and a quarter of the 116 allergologists in the entire country practice in this area. This region likewise hosts the greatest number of tertiary hospitals and specialist training institutions where access to CME activities is generally high. This would explain the high awareness of and adherence to guidelines on AR of specialist physicians in the NCR.
Based on self-reported perception, there is sufficient level of knowledge regarding AR among both groups. The finding that more specialists compared to generalists believe they have more adequate knowledge on AR can be partly attributed to the former's attendance to a greater number of CME activities. On the average, specialists attend 3 CME activities compared with 2 for the generalists; the difference is significant (p < 0.05). All respondents believe that CME activities are helpful and applicable to their practice. Both groups cite triggers of AR as the single most important topic for CME activities. Elimination or control of triggers is appealing for Filipino patients as they may be effective, easier to perform, cheaper, and safe. Allergen avoidance, however, may be difficult to implement in the Philippines. Like most developing countries, the population is exposed to more allergens and irritants because of the adoption of a Western lifestyle, rapid industrialization, and a high pollution index [2]. The respondents agree that there is a need to discuss topics related to national data on AR. Predominant circulating allergens are unique for each country and local studies on these are believed to be urgently needed. Likewise, both groups strongly share the belief that most patients are not knowledgeable about AR and need to be educated about the disease.
Asthma is the most common comorbid condition of AR seen by both groups. It is reported that 60-80% of patients with asthma have concomitant AR in the Asia-Pacific region. Compared to other regions in the world, these rates are higher [13]. Specialists also report managing more patients with concomitant rhinosinusitis compared to generalists.
Both groups report adherence to AR guidelines. For respondents who follow guidelines, most use ARIA. However, a greater percentage of specialists know the meaning of and follow ARIA recommendations. General practitioners have a greater patient load and may have difficulty implementing AR guidelines. Reasons for this may include inadequate organization in practice, skepticism on guideline effectiveness, and problems related to integrating evidence-based medicine with daily practice [14]. It is also reported that attendance to CME activities correlates with better adherence to guidelines as this facilitates better understanding and promotes a higher level of confidence among physicians [15]. Our data shows a statistically significant difference in CME attendance between the two groups.
Majority of the physician respondents do not routinely use diagnostic tests for AR. This finding is consistent with reports from other studies [1617]. In the Philippines, the national health insurance program (PhilHealth) coverage for the NCR is pegged at 54.7% of the population [18]. PhilHealth does not have full coverage for ancillary AR procedures. Therefore, diagnostic procedures are mostly out-of-pocket expenditures for patients. Of the specialists who use diagnostic tests, otolaryngologists prefer nasal endoscopy while allergologists prefer skin tests. This is to be expected as these are the physicians trained and highly skilled in performing such procedures.
Both general and specialist physicians manage patients with mild AR. However, more specialists manage moderate-severe AR. Generalists prefer to send patients with severe, complicated or recalcitrant disease to specialists. The Philippine healthcare structure also allows patients to bypass GPs and directly seek consult with specialist physicians. Especially for those who pay out-of-pocket for healthcare, this system allows patients to save on consultation fees, transportation costs, and wait-time between consultations.
Monotherapy, specifically an oral second generation antihistamine given for 7 days, is the preferred first line of treatment for mild AR by both groups. This management is consistent with the ARIA guidelines where second generation antihistamines are recommended for mild AR as monotherapy. For the minority who use combination therapy, the preferred drug combination is an oral second generation antihistamine given for 7 days plus an oral decongestant given for 5 days. Although this is not recommended by ARIA, the guidelines state that oral antihistamine-decongestant combination may be beneficial for some patients as a rescue medication, given the minimal effects of decongestion obtained from antihistamines. In this study, physicians prescribe oral decongestants for a maximum of 5 days to minimize the adverse events associated with its use.
For the management of moderate-severe AR, both groups are equally divided among those who use monotherapy and those who prefer combination therapy. The preferred monotherapy of both groups is an INCS given for one month. For those who use combination therapy, half prescribe an oral second generation antihistamine with antileukotriene; the rest use INCS, oral second generation antihistamines, and antileukotrienes. These protocols are also consistent with ARIA recommendations for moderate-severe AR.
Both groups of physicians cite efficacy as the primary reason for their choice of therapy for the management of mild or moderate-severe AR. For mild AR, the generalists prefer antihistamines because these provide "relief of general symptoms". Specialists cite "relief of general symptoms" and long duration of action as the reasons for their preference for antihistamines. For moderate-severe AR, both groups cite efficacy as the primary reason for their preference for INCS. The preferred use of branded drugs by both groups may be partly explained by the perception that these have a greater efficacy compared to generic drugs. Other reasons cited for preference for a particular drug are "inclusion in guideline recommendations" and cost. Cost is an important consideration for Filipino physicians because most patients pay out-of-pocket for AR drugs. Both groups cite "economic reasons" as the most common reason for noncompliance of patients with treatment. Generic or innovator drugs in the Philippines are more expensive compared to other Asia-Pacific countries with similar Gross Domestic Product. The difference in drug pricing is due to import levies, mark-ups from wholesalers, distributors, pharmacy outlets, and imposition of a value added tax on pharmaceutical products [19]. Nevertheless, the choice of therapeutic regimens shows that both general and specialist physicians prioritize efficacy over cost.
For adjunctive therapy, most general physicians prefer multivitamins; specialists prefer nasal saline douche/irrigation. Currently, there is weak evidence to support the role of vitamins in allergic disease [20]. Studies show that use of nasal saline irrigation results in a significant decrease in nasal symptom scores, better mucociliary clearance, and improved quality of life. It is also noted to be economical, easy to use, and safe for long-term use. However, controversies exist regarding optimal saline concentration and method of delivery for optimum nasal symptom control [21].
In conclusion, despite differences in awareness of and adherence to guidelines on AR, prescribing patterns on management of mild and moderate-severe AR are similar among Filipino general and specialist physicians. This can be attributed to a shared perception of efficacy and cost as the drivers for choice of therapeutic regimens.



 XML Download
XML Download