

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
House dust mites (HDMs) are important sources of indoor allergens [1]. In the general population, the prevalence of HDM sensitization is 9-16% [2]. More than 10 different species have been found in house dust, three of which are very common worldwide-Dermatophagoides pteronyssinus (Der p), Dermatophagoides farinae (Der f), and in tropical climates, Blomia tropicalis [3].
Currently, 17 HDM components have been identified from Der p [45] and Der p 1 and Der p 2 are known to be major allergens [6].
Three groups of HDM proteins are currently available for routine laboratory work-up of HDM sensitized patients. Group 1 mite allergens (Der p 1 and Der f 1) are cysteine proteases with multiple effects on mite-host interaction. These proteases facilitate allergen delivery to the submucosa and its antigen-presenting cells, leukocyte recruitment and activation, including mast cell and eosinophil degranulation, bronchial smooth muscle contraction and proliferation [78910]. Group 2 mite allergens (Der p 2 and Der f 2) are molecular mimickers of MD-2, a lipopolysaccharide coreceptor for the toll-like receptor-4 [1112], thus interacting with the innate immune system [478]. Der p 10 (tropomyosin) is a minor HDM allergen, but its highly homologous counterparts in seafood and snails are well-known inducers of severe systemic anaphylaxis [1314].
It has been previously shown that serum Ig E to Der p groups 1 and 2 are highly prevalent in HDM allergic patients. While Ig E to Der p 10 is often associated to broader sensitization, such as food [131516]. Still, important variations in Der p 1 (64-100%), Der p 2 (62-91%) and Der p 10 (6-59%) IgE prevalence are reported, which may be accounted for by geographical, age and clinical status-related differences in the study populations [171819202122].
Our aim was to define the prevalence of IgE to Der p 1, Der p 2, and Der p 10 in Korea and investigate the clinical features of them in children with allergic disease.
MATERIALS AND METHODS
We performed a prospective evaluation of 80 newly diagnosed HDM sensitized allergic patients presenting to the outpatient allergy clinic of the Seoul St. Mary's Hospital in Seoul, Korea between April 2013 and March 2014. The study was approved by the Seoul St. Mary's Hospital Institutional Review Board Committee (protocol No. KC13TISI0511).
Patients
During the study period, 153 children who visited the Allergy Clinic of Seoul St. Mary's Hospital had documentation of clinical criteria sufficient for the diagnosis of atopic dermatitis (AD), allergic rhinitis (AR), asthma (AS), or urticaria (UC). These patients were offered a screening medical examination; in vitro specific IgE measurements against Der p, Der f (ImmunoCAP, Pharmacia Diagnostics AB, Uppsala, Sweden) or MAST OPTIGEN allergy system (Hitachi Chemical Diagnostics, Mountain View, CA, USA). Patient guardians expressed written informed consent and were followed up at the clinic periodically.
MAST OPTIGEN
Patient sera were added to MASTpette chambers which contain 35 kinds of allergens including food and inhalant. After 2 hours of incubation and washes, enzyme-tagged anti-IgE was added. After 2 hours of incubation and washes, luminescent reagent was added. After 10 minutes of incubation, results were interpreted as class 0-4 with MAST OPTIGEN luminometer. Class ≥ 1 was interpreted as positive.
HDM sensitized patients
Patients presented with ≥ 0.35 IU/mL serum levels of IgE to Der p crude extract or Der f crude extract by ImmunoCAP or class ≥ 1 to Der p or Der f by MAST OPTIGEN were defined as sensitized to HDM. As a result, eighty HDM sensitized patients underwent ImmunoCAP for total IgE, Der p, Der f, Der p 1, Der p 2, and Der p 10. Sensitization to Der p, Der f, Der p 1, and Der p 2 were considered significant when specific IgE was >0.35 IU/mL and patients with Der p 10 specific IgE higher than 0.1 IU/mL were considered to be sensitized.
Clinical diagnostic criteria
For the diagnosis of AR: a symptomatic period of minimum 2 months, with at least two of the following: watery rhinorrhea, blocked nose, itchy nose, sneezing, or night cough [23]. For the diagnosis of AD: we used the age appropriate clinical criteria for allergic eczema in childhood, summarized by Muraro et al. [24]. For the diagnosis of AS: a previous diagnosis of AS with proof of reversibility on pulmonary function tests and response to bronchodilators. With younger children or where such evidence was not readily available: a history of three or more episodes of at least two of the following - persistent day time or night time cough, doctor-diagnosed nonfebrile wheezing, recurrent episodes of shortness of breath or exercise-induced shortness of breath or cough. UC defined as a disease characterized by the development of wheals (hives), angioedema, or both [25]. These data were obtained from the clinical records, their clinic interview, and medical examination.
Mite component-specific IgE in serum
Total IgE levels, specific serum Ig E Der p crude extract, Der f crude extract, Der p 1, Der p 2, and Der p 10 were measured with the ImmunoCAP immunofluorimetric assay, components and reagents (Thermo Fisher Scientific, ImmunoDiagnostics, Uppsala, Sweden). Measures of total IgE levels were expressed in international units per unit volume (IU/mL, 1 IU equals 2.4 ng). Specific IgE levels were expressed in arbitrary units per unit volume (IU/mL). The measuring range of total IgE was between 2 and 5,000 IU/mL and that of specific IgE to Der p extract and molecular components was between 0 and 100 IU/mL. In case a measure was too high for the measuring range, we assumed IgE to be 100 IU/mL. The ImmunoCAP 250 machine underwent monthly quality controls (Euro EQAS for Total IgE, Euro EQAS for Specific IgE, Phadia Quality Club for specific IgE).
Statistical analysis
For each patient, levels of total and specific IgE were expressed as previously described. For patient groups, levels of total and specific IgE were expressed as the mean ± standard deviation. Prevalence of Der p, Der f, Der p 1, Der p 2, and Der p 10 sensitizations were expressed with confidence intervals. Comparisons of prevalence in different group were done with Wilcoxson rank sum test for continuous variables. Correlations between total IgE and the antibody responses were analyzed by Spearman rank correlation test. Association between antibody responses and allergic disease were analyzed by chi-square test, Fisher exact test and Wilcoxson rank sum test. All statistical analyses were analyzed using SAS ver. 9.3 (SAS Institute Inc., Cary, NC, USA) and p value of less than 0.05 was considered statistically significant.
RESULTS
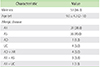
During the study period, 153 children who visited the Allergy Clinic of Seoul St. Mary's Hospital had documentation of clinical criteria sufficient for the diagnosis of AR, AD, AS, or UC. Of the 153 patients, 19 patients were sensitized to food allergens and 95 patients were sensitized to aeroallergens. Within the 95 patients sensitized to aeroallergen, 80 were found to be sensitized to HDM and considered to be the study population. The study population consisted of 53 males and the mean age was 9.0 ± 4.3 years (range, 2.0-18.0 years). There was 1 case of AD, 31 cases of AR, 36 cases of AS, 4 cases of UC, 4 cases of AD and AR, 3 cases of AR and AS, and 1 case of AR and UC. Clinical severity was mild to moderate in all patients (Table 1).
Prevalence and levels of specific IgE to Der p, Der f, Der p 1, Der p 2, and Der p 10
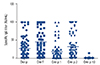
Seventy-nine patients (98.8%) had detectable serum IgE to Der p, 80 patients (100%) were sensitized to Der f, 66 patients (82.5%) were sensitized to Der p 1, 63 patients (78.8%) to Der p 2, and 7 patients (8.8%) were sensitized to Der p 10 (Fig. 1).
In respect to allergic disease, IgE reactivity to Der p 1 was significantly lower in the UC group compared with the AD group and the AR group (Fig. 2).
Der p 10 sensitized patients
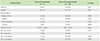
Seven patients (8.8%) reacted to Der p 10. Six patients were male and their mean age was 7.6 ± 2.9 years. There were 3 cases of AR, 4 cases of AS, 1 case of AD (Table 2). In comparing Der p 10 sensitized group and the rest, total IgE was significantly higher in the Der p 10 sensitized group (p = 0.042) (Table 2). Der p 10 serum IgE level was highly correlated with serum IgE level to crab and shrimp (p < 0.0001 and p < 0.0001, respectively) (Fig. 3). Cockroach showed no correlation with Der p 10 specific IgE (p = 0.670) (Fig. 3).
Correlation between total IgE and specific IgE to HDM and its components
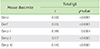
We found a moderate positive correlation between total IgE and specific IgE to Der p, Der f, Der p 2, and Der p 10 and low positive correlation between total IgE and Der p 1 specific IgE (Table 3).
DISCUSSION
HDM are major allergen sources for almost 50% of allergic patients [26]. In this study, we aimed to define the prevalence of sensitization to Der p 1, Der p 2, and Der p 10 components and investigate the clinical phenotype in allergic children. In our study, the prevalence of sensitization to Der p was 98.8%, Der f was 100%, Der p 1 was 82.5%, Der p 2 was 78.8%, and Der p 10 was 8.8%. Patients with UC had significantly lower IgE titer to Der p 1 than AD and AR. Patients sensitized to Der p 10 showed a significant positive correlation with IgE to crab and shrimp. Total IgE showed significant positive correlation with Der p, Der f, and its components.
Prevalence of HDM sensitization has been studied previously in various climates. According to a study involving French children in 2012, prevalence of Der p 1 sensitization was 95%, Der p 2 was 75%, and Der p 10 was 30% [27]. In another study involving Austrian children and adults, the prevalence of Der p 1 sensitization was 91%, Der p 2 was 86%, and Der p 10 was 6% [17]. Another study conducted in Singapore, which has a tropical climate, reported Der p 1 sensitization prevalence of 64%, 71% showed sensitization to Der p 2, and Der p 10 was sensitized in 4% of the study population [19]. In our study, Der p 1, Der p 2, and Der p 10 sensitization rates were similar to previous studies from temperate climate. The strongpoint of our study lies in the fact that ImmunoCAP was used to determine specific IgE. Previous studies usually used allergen dot immunoblot arrays that are known to be prone to nonspecific IgE binding as well as nonspecific inhibition of IgE binding by the presence of large quantities of antigen specific IgG in patients sera [1728].
Because Der p 1 and Der p 2 play distinct pathophysiological roles, we hypothesized that sensitization to Der p 1 and Der p 2 specific IgE might influence the clinical phenotype. Therefore we examined for any association between component-specific IgE sensitization with diagnosis of allergic disease. Der p 1 specific IgE titer was significantly lower in the UC group compared with AD group and AR group. This was similar to previous studies which found no particular pattern of component-specific IgE sensitization associated with individual diagnosis of allergic disease, such as AD, AR, and AS [1927]. However, we found that UC group had significantly lower Der p 1. Further studies involving midrange prevalence molecular components such as Der p 4, Der p 5, and Der p 7 might help clarify the reason for such differences [21].
Der p 10 (tropomyosin) is a minor mite allergen but prominent in seafood, and cross-reactivity is extremely frequent [29]. As expected, in our study, the Der p 10 specific IgE had a significant positive correlation with the specific IgE to shrimp and crab. However, the Der p 10 specific IgE levels showed no correlation with the specific IgE titers to cockroach as previous studies described [3031]. Our results suggest that high-level Der p 10 IgE reactivity is might be associated with seafood allergy. One possible explanation might come from the high consumption of seafood in Korea, influencing tropomyosin IgE reactivity [31]. Der p 10 sensitized patients had significantly higher total IgE titer compared with Der p 10 nonsensitized group. Further study will be needed to determine its precise significance.
Finally, quantitative data showed a strong correlation between serum levels of total IgE and specific IgE to crude extract of Der p, Der f and its components, Der p 1, Der p 2, and Der p 10. Total IgE was a very good predictor of the levels of Der p, Der f, Der p 1, Der p 2, and Der p 10 IgE levels. Therefore the measurement of serum levels of IgE to Der p 1, Der p 2, or Der p 10 brought little additional information in patients already tested for Der p.
Our study had a few limitations. First, the study was a cross sectional study therefore causal relationship between phenotypic expression and sensitization to HDM and its components were hard to determine. Secondly, the study population was selected from a tertiary hospital located in an inner city environment resulting in selection bias. Finally, we could not perform oral food challenge in children who showed high levels of IgE to shrimp or crab to confirm the diagnosis of food allergy.
In conclusion, sensitization to HDM and its components in Korea is similar to previous studies from temperate climate. The determination of Der p 1, Der p 2, and Der p 10 IgE helps in obtaining additional information in regards to allergic disease. However, cost-benefit aspect should be considered.


 XML Download
XML Download