

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Bronchial asthma is the most common chronic condition in children and adolescents worldwide, affecting around 300 million patients, and the prevalence is continuing to rise [1]. Asthma is caused by excessive and inappropriate immune responses to environmental antigens. As an immune-mediated disease, asthma is characterized by reversible small airway inflammation leading to episodes of wheezing and respiratory distress [2]. Several factors are involved in suboptimal control of asthma in children like positive atopic status, exposure and sensitization to environmental allergens and/or familial history of allergic disease [3]. This has led to the investigation of the immuno-modulatory properties of vitamin D as an anti-inflammatory agent for the management of asthma [4].
In fact, the importance of vitamin D in health and disease has been documented in literature beyond its known role in calcium metabolism and bone health [5]. Furthermore, reduced vitamin D levels in adult and pediatric patients with mild-to-moderate asthma are associated with impaired lung function, increased airway hyperreactivity, and reduced corticosteroid response [6]. A threshold effect at serum vitamin D levels of at least 20 ng/mL (50 nmol/L) was suggested to be adequate in asthmatic children to attenuate the risk of exacerbations, while higher levels may not provide any additional benefits [7]. Nevertheless, there are uncertainties in defining the appropriate vitamin D cutoffs for respiratory health [8].
It has been reported that vitamin D deficiency is very common among Saudi children and adolescents [9, 10, 11]. However, little is known about vitamin D levels and their impact on disease control in Saudi children with asthma.
Therefore, we hypothesized that children with asthma have lower serum vitamin D levels than nonasthmatic controls and that lower vitamin D levels are associated with more severe asthma. The aim of the current study was to investigate the relationship between vitamin D levels and markers of asthma severity.
MATERIALS AND METHODS
A total of 70 Saudi boys and girls aged 4-18 years were sequentially recruited from the King Abdul Aziz University Hospital (KAUH), Jeddah, Saudi Arabia, over the period of 11 months (May 2011-April 2012). Forty-five asthmatic children were recruited from the Paediatric Pulmonary Department whereas 25 nonasthmatic controls were enrolled from the general health clinic. Ethical approval was obtained from the Research Ethics Committee of the KAUH. In addition, informed written consents to participate in the study were signed by the parents or the legal guardians of the studied subjects.
Subjects with chronic conditions such as pulmonary conditions (e.g., cystic fibrosis or bronchiectasis), malabsorptive syndromes, cancer, kidney or liver disease, previous diagnosis with developmental delay, and those taking calcium, vitamin D or multivitamin supplements were excluded from the study. Physical examination was carried out by the attending physician who ensured that the participants met the inclusion and exclusion criteria.
The study subjects were divided into 4 groups: the first group included 15 controlled asthma subjects, the second group included 15 partly controlled asthma subjects, 15 uncontrolled asthma subjects in the third group and 25 apparently healthy subjects in the fourth group (control).
A structured questionnaire was interviewer-administrated to all study subjects and/or their parents regarding their demographic characteristics personal medical history, and current asthma medications (controller and/or reliever). Data also included questions about family history of asthma, allergic rhinitis, and eczema. The use of the prevalidated childhood asthma control test (C-ACT) instrument was employed to assess the level of asthma control among asthmatic patients [12], as endorsed by the Saudi Initiative for Asthma management (SINA) panel [13]. The C-ACT instrument asks about the patient's activity limitations, shortness of breath, frequency of night symptoms, use of rescue medication and a rating of overall control of the disease over the past 4 weeks. The score of the C-ACT is the sum of 5 questions, where each is scored from 1 (worst) to 5 (best), leading to a maximum best score of 25. A score ≥20 indicates controlled asthma, scores from 16 to 19 indicate partly controlled asthma, and scores <16 indicate uncontrolled asthma.
Weight and height were recorded to the nearest 0.2 kg and 0.5 cm, respectively, using an appropriate international standard scale (Digital Pearson Scale, ADAM Equipment Inc., Danbury, CT, USA). BMI was derived using the formula weight (kg)/height (m2). Body mass index (BMI) <5th percentile was considered underweight, 5th-85th percentile was considered normal weight, 85th-95th percentile as overweight, and >95th percentile as obese [14].
Pulmonary function test was performed by a spirometer, as per American Thoracic Society standards [15], by recording changes in the peak expiratory flow (PEF), and C-ACT score. Asthma symptoms severity was assessed in accordance with the Global Initiative for Asthma (GINA) guidelines [1].
Allergic sensitization was ascertained by skin prick testing; dust, nuts, milk products and egg (Bayer, Elkhart, IN, USA); sensitization was defined as wheal diameter of at least 3 mm greater than the negative control to at least one of the standard allergens.
Venous blood samples were withdrawn from all study participants. Bone profile parameters, including serum levels of albumin, calcium, phosphate, magnesium, alkaline phosphatase activity level, were measured using standard analytical techniques (Ortho Clinical Diagnostics Inc., Rochester, NY, USA). Serum calcium was adjusted for albumin; corrected serum calcium = [serum calcium (measured) + 0.8 × (4-serum albumin)]. Electrochemiluminescence Immunoassay kit was used to measure serum 25-hydroxyvitamin D levels (Roche Diagnostics GmbH, Mannheim, Germany). Vitamin D deficiency was defined as serum 25-hydroxyvitamin D less than 50 nmol/L and serum levels between 50-75 nmol/L were defined as insufficient whereas vitamin D sufficiency was considered between 75-100 nmol/L [16].
Cytokines profile levels (interleukin-10 [IL-10], tumor necrosis factor-alpha [TNF-α], platelets derived growth factor [PDGF]) were measured by enzyme-linked immunosorbent (ELISA) assay kit (Cell Applications Inc., San Diego, CA, USA). Total IgE antibodies levels were determined using the ELISA method (R-Biopharm AG, Darmstadt, Germany).
The peripheral blood eosinophil's cell count was measured using Coulter counter techniques (Coulter AcT diff2 Analyzer, Beckman Coulter Inc., Brea, CA, USA). The absolute count of eosinophil was calculated as the product of its percentage and the total leukocyte count.
Continuous data were presented as mean ± standard error of mean for normally distributed data and as median (interquartile range) for nonnormally distributed data. Categoric data were expressed as number (percentage). Correlations were assessed by Pearson correlation (normal data) or Spearman rank correlation (skewed data). Categorical data were compared by chi-square test. Analysis of variance or Kruskal-Wallis test, was done to compare the subgroups depending on their distribution, followed by Bonferroni post hoc test for multiple comparison between the subgroups.
Stepwise linear regression analysis was done to determine which among the parameters measured are significant predictors for 25-hydroxyvitamin D (dependent variable). A p-value less than 0.05 was significant. Statistical analysis was carried out using the PASW Statistics ver. 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
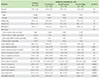
Clinical characteristics of the study participants are summarized in Table 1. There were no significant differences between children with asthma and nonasthmatic control subjects in age, gender distribution, or BMI value (p>0.05).
Asthmatic children showed significantly higher serum levels of all cytokines and atopy markers than nonasthmatic controls (p<0.0001). However, when asthmatic children were divided according to the level of asthma control, lower serum levels of IL-10 were detected among partially controlled and uncontrolled asthmatics in comparison with controlled asthmatic children (p<0.05). Similarly, higher serum TNF-α levels and eosinophils count were observed among par tially controlled and uncontrolled asthmatics as compared with their counterparts' controls (p<0.05). Whereas, only uncontrolled asthmatics had significantly lower serum levels of platelet derived growth factor (PDGF) than controlled asthmatics (p<0.05).
In this study, asthmatic patients were classified into 3 subgroups based on the level of asthma control as defined by the C-ACT score (Fig. 1A), as this was thought to be the best approach to control for the effect of asthmatic medication.
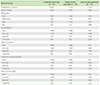
Table 2 shows the severity of asthma symptoms among the study patients as assessed by the GINA guidelines. Over two thirds of the asthmatic children had familial history of asthma and were complaining from different allergies. About 46% of the asthmatic patients were allergic to dust whereas 33% had various food allergies.
Fig. 1B demonstrates that PEF rate in uncontrolled asthmatic is significantly lower than controlled asthmatic and those with partial control of asthma symptoms (p<0.0001).
Fig. 2 summarizes serum vitamin D levels among asthmatic patients as divided by the severity of asthma symptoms. Children with uncontrolled asthma had significantly lower median 25-hydroxyvitamin D serum levels (18.5 nmol/L) as compared to controlled (52.7 nmol/L) and partially controlled asthmatic children (33.3 nmol/L) (p<0.0001).
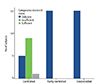
Fig. 3 displays asthmatic children classification according to vitamin D status. In controlled asthmatics, the prevalence of vitamin D insufficiency was 7%, with 93% being vitamin D deficient. All uncontrolled asthmatic children and asthmatics with partial control were vitamin D deficient.
There was a positive correlation between serum 25-hydroxyvitamin D levels and asthma symptoms (C-ACT score) (r = 0.956, p < 0.0001) whereby higher serum 25-hydroxyvitamin D was associated with better asthma control, and lung functions (PEF rate) (r = 0.962, p < 0.0001). No significant relationship was shown between serum levels of 25-hydroxyvitamin D and IgE and eosinophils count (Table 3).
Fig. 4 depicts correlation analysis of serum vitamin D with cytokines profile among the study population. Serum 25-hydroxyvitamin D levels were positively associated with PDGF (r = 0.313, p < 0.05) and with the anti-inflammatory cytokine IL-10 (r = 0.868, p < 0.0001). Furthermore, an inverse correlation was noted between serum 25-hydroxyvitamin D levels and TNF-α levels (r = -0.450, p < 0.0001).
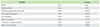
To adjust for possible confounding variables, multivariate analysis was carried out. Stepwise variable inclusion with p < 0.05 and exclusion with p > 0.10. These include BMI, weight, TNF-α, and PDGF. Table 4 shows that 95% of the changes in serum vitamin D levels can be explained by 3 major determinants among the study population of asthmatic children: serum IL-10 (β = 0.575, p < 0.0001), PEF rate (β = 0.785, p < 0.0001), and C-ACT score (β = -0.337, p < 0.01).
DISCUSSION
In spite of significant improvement of treatment options and diagnostic tools, asthma remains in many patients uncontrolled [3]. In Saudi Arabia, environmental factors are thought to play a major role in the etiology of bronchial asthma whereas genetic factors are considered to be less important [17, 18]. Among which, nutritional status acts a vital role [19]. This was obvious in our study population with 20% of the controlled asthmatics being underweight whereas 47% of uncontrolled asthmatics were obese.
While many nutritional factors could account for the etiology of asthma, vitamin D deficiency has been proposed as a risk factor that could explain a significant proportion of increased pattern of asthma prevalence [20]. Vitamin D deficiency is becoming an important public health problem in many countries with abundant sun exposure [7, 9, 10, 11]. Hypovitaminosis D was highly prevalent in our study population with 78% are considered vitamin D deficient. Similar studies from other countries revealed similar results [7, 21] that can be explained by ethnicity, skin color and maternal supplementation during pregnancy. Therefore, it is necessary to increase the vitamin D dose, the period of exposure to sunlight, the time of exposure to sunlight (preferably around midday), in addition to the use of sun blocks, and protective clothing [5].
Furthermore, univariate analysis demonstrated inverse correlations between weight, BMI, and serum vitamin D levels (Table 3). These findings are consistent with prior data [6 ,22].
Vitamin D deficiency and asthma development
It has been shown that, in addition to affecting immune cells, vitamin D affects smooth muscle function and proliferation, which has a direct relevance for lung function in asthma and in airway remodeling [23]. The current study demonstrated a significant relation between the deficiency of vitamin D and the severity of asthma (Fig. 2) (p<0.05). Thereby, conceding with previous reports of asthmatic children with low serum level of vitamin D having a greater risk of suffering severe asthma attacks than those with higher levels of the vitamin [24].
Additionally, vitamin D deficiency has been linked to an increased incidence of asthma in children [20, 25]. This was demonstrated in our study with C-ACT score being a strong independent determinant of circulating vitamin D levels (β = -0.337, p < 0.01, 95% confidence interval [CI], -1.040 to -0.184). This is in agreement with the work conducted by Bener et al. [7], who confirmed that vitamin D levels were predictive of asthma and allergy outcomes. C-ACAT instrument is considered responsive to changes in the patient clinical status over time when used for treatment maintenance and adjustment [12]. Furthermore, tailoring asthma treatment to the level of actual disease control and future risk has been implemented in SINA guidelines [13].
Vitamin D deficiency and pulmonary function
Vitamin D involvement in the metabolism and function of tissues other than bone is increasingly documented [26, 27]. Vitamin D status is correlated with lung function [6]. Furthermore, a dose-dependent association between lower serum 25-hydroxyvitamin D and reduced pulmonary function [28]. In our study, PEF rate, as a measure of lung function, was also a strong determinant of circulating vitamin D levels (β = 0.785, p < 0.0001, 95% CI, 0.074-0.131). This is in agreement with previous findings of vitamin D deficiency predisposition to decreased lung functions and poor asthma control [22, 29, 30].
Vitamin D deficiency and asthma disease severity
Lower levels of vitamin D in children were associated with increased markers of asthma severity [29]. Our results demonstrated that hypovitaminosis D is correlated with reduced asthma control, indicated by higher number of asthmatic episodes, worsen daytime symptoms, limitation of the outdoor activities, and increased need to use inhaler (Table 3).
Many studies suggest that vitamin D may have therapeutic potential in severe asthma patients as a steroid-enhancing agent [31, 32]. Among the vitamin D-stimulated processes that contribute to tolerance are induction of dendritic cells, development of T cells, activation of T-cell and antigen receptor signalling, and elaboration of anti-inflammatory cytokines, including IL-10 [33]. It was recently shown that 1,25-dihydroxyvitamin D significantly increased the secretion of IL-10 and decreased the secretion of IL-6 and IL-17 by immune cells [34]. Addition of 1,25-dihydroxyvitamin D leads to decreased secretion of IL-2 and interferon-γ by CD4 T cells and promotes IL-5 and IL-10 production, which further shifts the T-cell response towards Th2 dominance. Serum IL-10 was also shown to be a predictor of circulating vitamin D levels in our study (β = 0.575, p < 0.0001, 95% CI, 1.290-1.991). It is therefore plausible that the link between reduced IL-10 levels and lung function in severe asthma may partly be explained by hypovitaminosis D levels.
Vitamin D deficiency in allergy sensitization
A relationship between inadequate vitamin D and development and severity of allergy has been proposed [28]. It was found that allergic sensitization to many allergens was more common in those with vitamin D deficiency (<37.5 nmol/L or 15 ng/mL) after multivariable adjustment. Sensitization included food allergens, indoor and perennial allergens, and pollen [35].
Our results are in agreement with the National Health and Nutrition Examination Survey in that asthmatic children with low serum vitamin D levels (<50 nmol/L or 20 ng/mL) are more likely to have food allergic sensitization (Table 2).
Vitamin D deficiency and atopy
Lower vitamin D concentrations have been found to be associated with higher risks of asthma exacerbations (e.g., hospitalization and use of anti-inflammatory medications) and increased levels of serum total IgE and peripheral eosinophil count in Costa Rican children with asthma [24]. This was also reproduced in the current study among asthmatic children irrespective of the degree of asthma symptoms control (Table 1). Nevertheless, no association was found between serum vitamin D levels and the quantified eosinophils inflammatory cells as well as serum IgE levels. This may be due to the small number of subjects in our study. Interestingly, not all investigators have found correlations between lower 25-hydroxyvitamin D levels and markers of allergy in childhood asthma [29]. It is possible that anti-inflammatory treatment prescribed for these children may have masked this relationship. However, it was suggested that vitamin D supplementation in children with low 25-hydroxyvitamin D levels may be a novel therapeutic target for asthma.
Vitamin D deficiency and immunity
Cytokines and chemokines play important roles in regulating the immune system. T-helper 1 (Th1) and Th2 cells were important regulators of the class of immune response. Several studies suggested that vitamin D deficiency could lead to immune malfunctioning [36]. Interestingly, TNF-α has been suggested as a new therapeutic target in subjects with severe asthma [37]. We have demonstrated an inverse relationship between vitamin D and TNF-α as a marker of asthma and allergy severity (Fig. 4). Our results support that vitamin D deficiency causes increase in the expression of TNF-α, thereby increasing inflammation and decreases the expression of vitamin D receptors (VDRs) [6]. Although the exact mechanisms of lower vitamin D levels in chronic inflammatory states are not yet elucidated in asthma, this deficit probably interferes with immunoregulatory functions of vitamin D. Immune cells (T and B lymphocytes, macrophages, and dendritic cells) express VDR and are affected by vitamin D deficiency during their maturation process. VDR may function as a regulator of asthma and atopy susceptibility [38]. Therefore, the addition of VDR involvement in the understanding of asthma/atopy pathogenesis will shed light on better control and treatment.
Vitamin D deficiency and inflammation
In chronic asthma, structural alterations of the airway characterized by airway smooth muscle (ASM) hypertrophy and hyperplasia [39]. Despite the use of glucocorticoids in the management of airway inflammation and hyperresponsiveness, there remains no specific therapy to prevent or inhibit ASM growth. It has been suggested that vitamin D supplementation might potentiate the anti-inflammatory function of corticosteroids in asthmatic patients [32]. Vitamin D may modulate airway inflammation and cell growth. Evidence suggests that alterations in vitamin D metabolism or supplementation with vitamin D may modulate airway inflammation or response to asthma therapy [4, 5, 20]. Our observation of a hypovitaminosis D association with increased asthma severity in asthmatic patients (Fig. 4) extends previous findings of in vitro studies. The precise signalling mechanisms by which calcitriol inhibited ASM cell growth remain unclear, but involved diminished hyperphosphorylation of retinoblastoma protein induced by PDGF and the phosphorylation of checkpoint kinase-1 [23, 40, 41].
Study limitations
We have investigated the association between vitamin D deficiency and the risk of asthma in Saudi children in a cross-sectional study design. However, the observational nature of the current study precludes the ability to discern temporal associations.
Also, we did not have detailed information on the socioeconomic status and lifestyle details (e.g., passive smoking history, duration of sunlight exposure) of the participants. Additionally, no objective markers of asthma (i.e., bronchial hyperresponsiveness or bronchodilator response) were obtained.
Another limitation is the small sample size (n = 70), and a study with a larger number of asthmatics may be required to verify our findings. However, despite a low sample size we were able to document strong, important relationships between 25-hydroxyvitamin D and asthma severity.
In conclusion, our study showed that hypovitaminosis D is highly prevalent in the whole population in addition to a highly significant increase in several markers of allergy and asthma severity among asthmatic children as compared with healthy control children. Significant correlations between several inflammatory and immunological markers and vitamin D levels were also found. Finally, lower 25-hydroxyvitamin vitamin D levels were associated with a higher asthma prevalence in multivariable analysis.
Further prospective studies examining the potential mechanisms of vitamin D in asthma pathophysiology and intervention studies aimed at using vitamin D supplementation in children with asthma are needed to elucidate the nature of this association.




 XML Download
XML Download