

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Asia is the world's largest and most populated continent. It covers 30% of the Earth's land area, and hosts 60% of the world's current population [1]. During recent decades, the Asian population has quadrupled, and the economy has enormously grown up [2]. Thus now, Asia is the world's most 'dynamic' region.
Asthma is a major chronic disease in Asia, like other continents [3, 4]. The prevalence of childhood asthma has continuously increased over the decades in Asia [5]. This increasing significance has been well reflected in the activity of asthma research in Asian countries, which has doubled during the last decade [6]. However, in Asian adults, the epidemiological burden of asthma is largely unknown this lack is quite in contrast to extensive and systemic research efforts ongoing for childhood asthma epidemiology such as the International Study of Asthma and Allergies in Childhood (ISAAC) projects in Asian children [5].
How prevalent is asthma in Asian adult community populations? Is asthma increasing in Asian adults too? If we extrapolate previous findings from Asian children or the European Community Respiratory Health Survey (ECRHS) [7], we might simply expect that asthma is also increasing among Asian adult populations. However, factors underlying the epidemiology are not uniform across different demographic groups; and thus, there should be many questions to be directly answered in this population.
Here we aimed to review the literature on the epidemiology, and to identify tasks to improve our understanding of asthma in Asian adult populations.
Go to : 
LITERATURE SEARCH
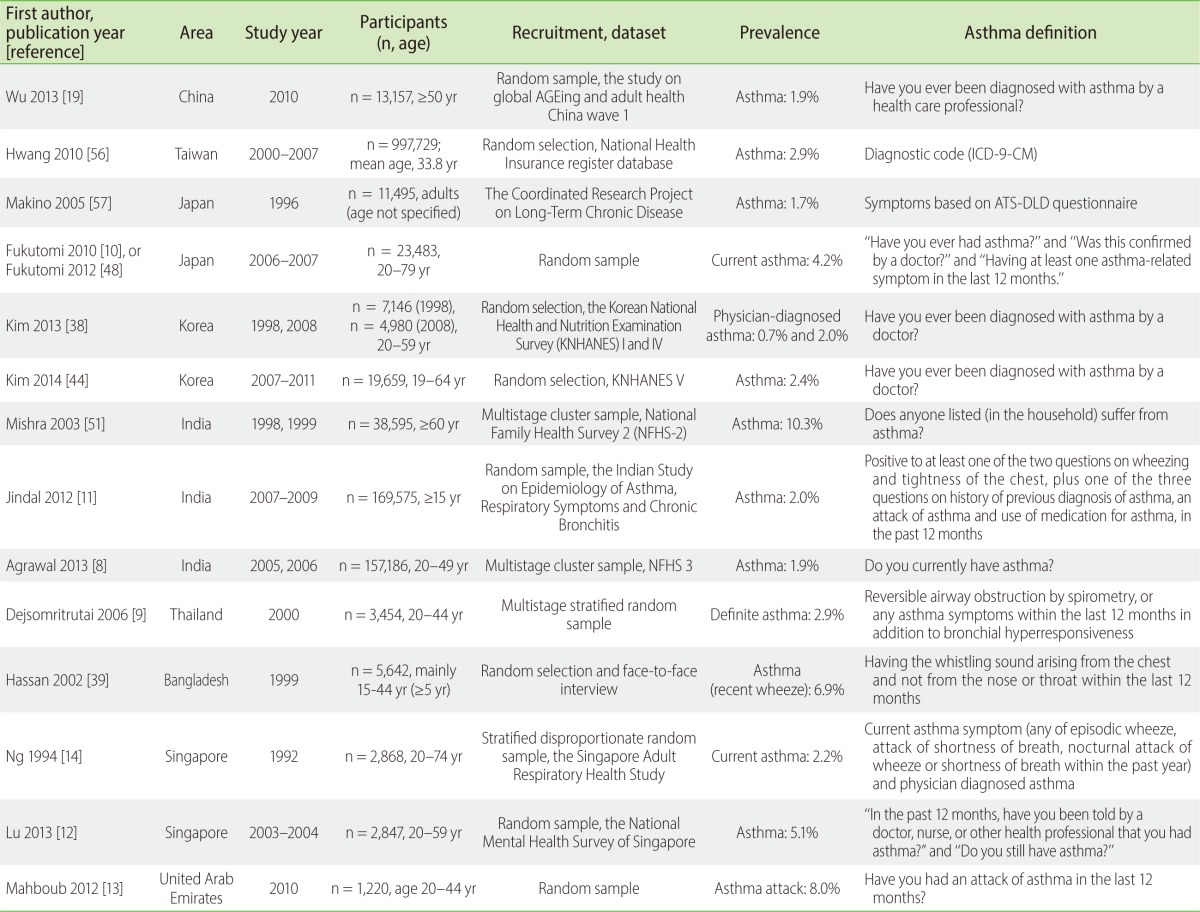
We conducted a semisystematic literature review to identify papers reporting the prevalence of asthma among Asian adult community populations. The PubMed was searched with the term 'asthma AND (epidemiology OR prevalence OR incidence)' for Asian countries. The publication period was not restricted, but the language was confined to English publication. Finally, we identified 42 original studies reporting the asthma prevalence in Asian adults. Outcomes were extracted for study design, population, research questions, case definition, and asthma prevalence (Tables 1, 2, 3).
Go to :
HOW PREVALENT IS ADULT ASTHMA IN ASIA?
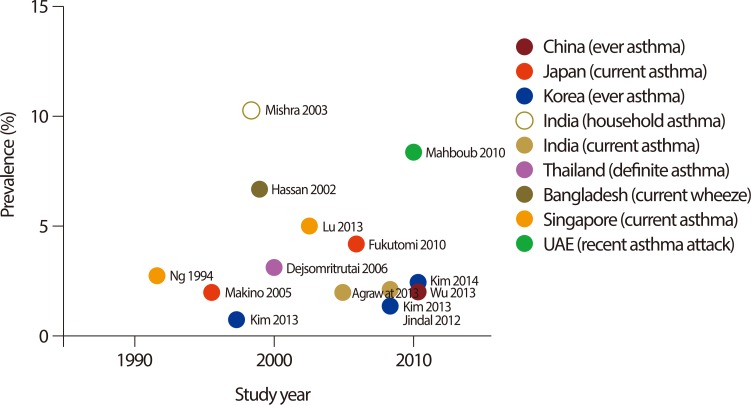
Prevalence data from nationwide surveys were summarized in Table 1. A total of 14 prevalence data have been reported from 9 countries. The prevalence varied from 0.7% to 11.9%, but the asthma definitions varied widely. Only one study had utilized objective testing (bronchodilator response) to define asthma, whereas others used questionnaires. Seven studies asked the 1-year prevalence of 'current asthma (defined by recent symptoms plus physician diagnosed asthma)' [8, 9, 10, 11, 12, 13, 14], but their definitions also varied between studies. These nationwide findings were depicted in Fig. 1.
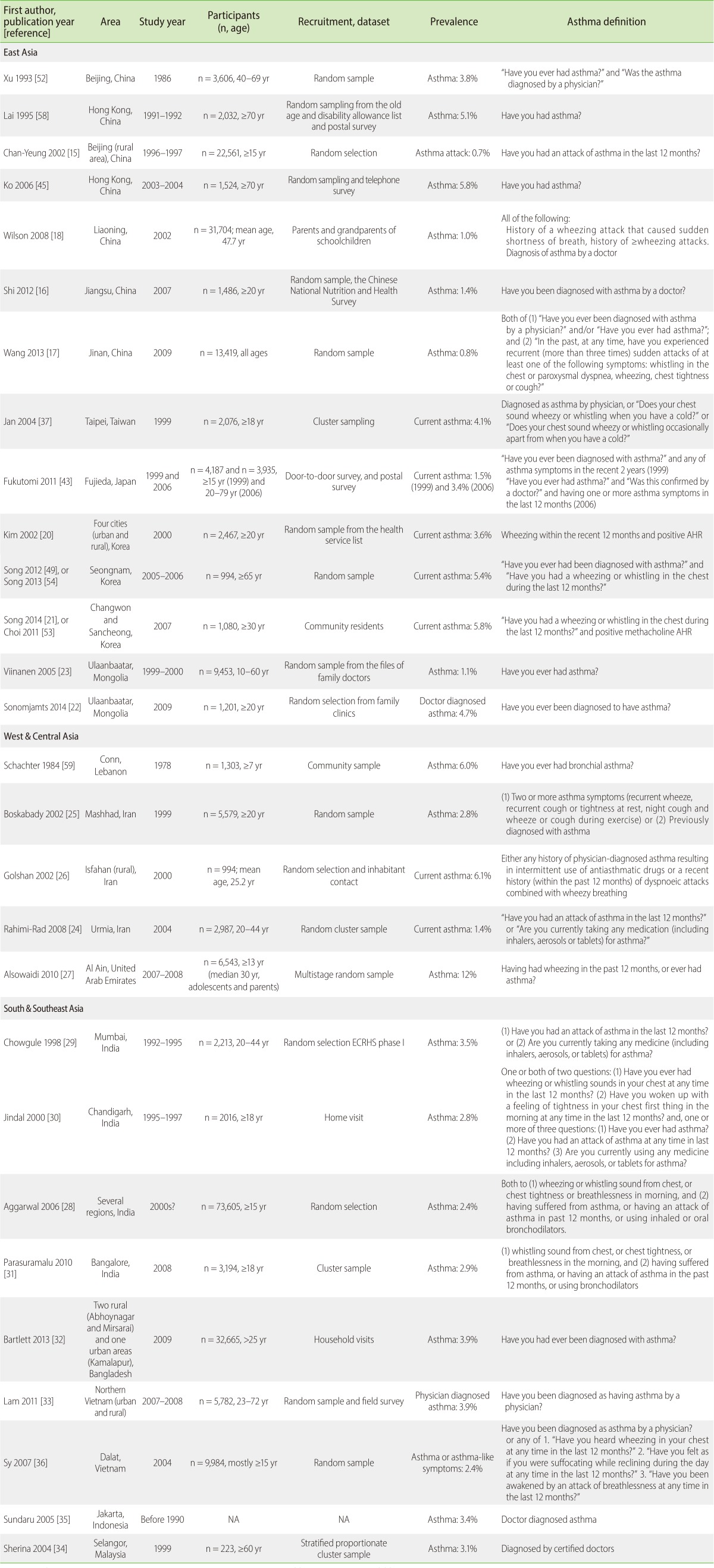
Local area surveys were summarized in Table 2 (28 studies from 13 countries). Specifically, local area prevalence in China was reported as 0.7-3.8% [15, 16, 17, 18, 19]. In two Korean local area studies, current asthma prevalence was 3.6-5.8% when defined by combination of questionnaire and methacholine challenge tests [20, 21]. In Ulaanbaatar, Mongolia, ever physician diagnosis of asthma varied from 1.1% in 1999 to 4.7% in 2009 [22, 23]. In Iran, three different local area surveys found current asthma prevalence as 1.4-6.1% [24, 25, 26]. In Al Ain, the United Arab Emirates, asthma prevalence was the highest as 12%, but the definition was not strict [27]. Four local area studies were conducted in India; the prevalence of current asthma ranged from 2.4% to 3.5% [28, 29, 30, 31]. Other South & Southeast Asian studies found 2.4-3.9% prevalence [32, 33, 34, 35, 36].
Interestingly, asthma was frequently reported to increase with aging in Asia. In two different local population surveys in Korea, current asthma (defined by current wheeze and positive airway hyperresponsiveness) was consistently more prevalent among the elderly (12.7-15.3%) [20, 21]. These age-related increase were similarly observed in several questionnaire-based studies from China [15, 17], Taiwan [37], Mongolia [22], Korea [38], Iran [25], India [8, 11, 28, 31], and Bangladesh [32, 39]. In Japanese nationwide surveys using questionnaires, only wheeze but not physician diagnosed asthma increased with aging [10]. The age-specific prevalence of asthma in elderly groups (≥60-70 years old) was presented in Fig. 2.

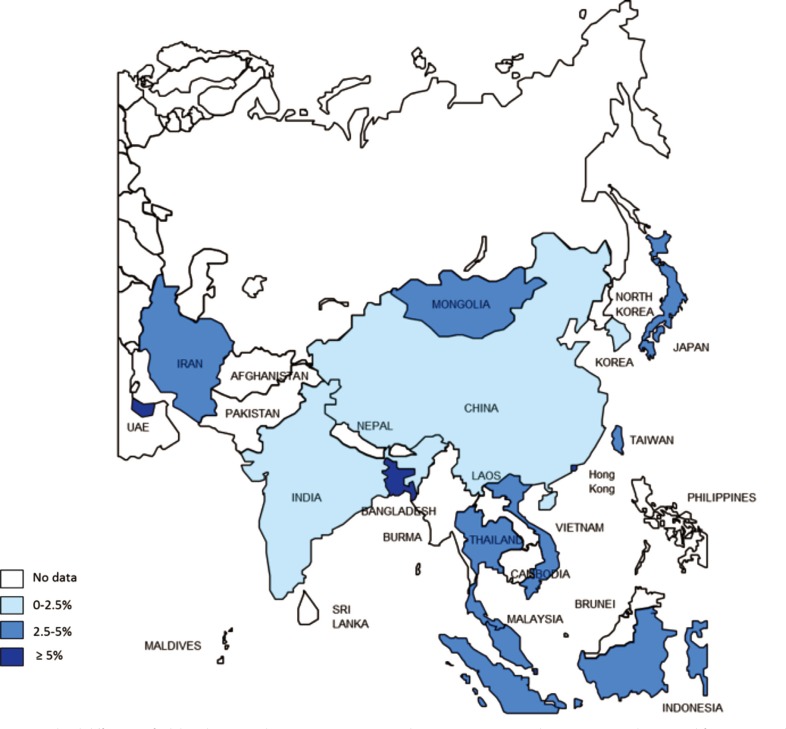
Despite the heterogeneity in study designs and years, we presented a crude prevalence map in order to have a quick glimpse of geographical variation of asthma prevalence in Asian countries (Fig. 3). Each representative prevalence was primarily retrieved from nationwide data, if available; otherwise, the pooled estimation from available local area studies was utilized as alternatives. To summarize, currently available data indicated that crude asthma prevalence was generally less than 5% in Asian adults. The Asian prevalence estimate was lower than the European data from the ECRHS phase I surveys (median, 4.5%; range, 2.0-11.9% in stage 1; and median, 5.2%; range, 1.2-13.0% in stage 2 [7]). These geographical difference between Asian and European populations were in line with the ISAAC surveys for childhood asthma [40].
Go to :
IS ASTHMA INCREASING IN ASIAN ADULTS?
In a recent systematic review, 48 well-designed cohort or repeated cross-sectional studies were analyzed to determine if asthma prevalence was declining recently (1990-2008) [41]. The analyses concluded that asthma prevalence recently continues to increase or remains stable in most parts of the world. However, the included studies were mostly childhood population studies, or from western populations, possibly due to lack of high quality longitudinal studies in Asian adult populations. In European adults, the ECRHS phase I and II comparison analyses (1991-1993 vs. 1998-2003) found the significant increase in 'asthma attack' (+0.8%; 95% confidence interval [CI], 0.2 to 1.4; p = 0.001), 'current asthma medication (+2.1%; 95% CI, 1.6 to 2.6; p < 0.001) or 'diagnosed asthma' (+2.2%; 95% CI, 1.6 to 2.9; p = 0.037), but no significant change in 'current wheeze' (-0.9%; 95% CI, -1.9 to 0.2; p = 0.122) over the 5- to 10-year follow-ups of young adults [42].
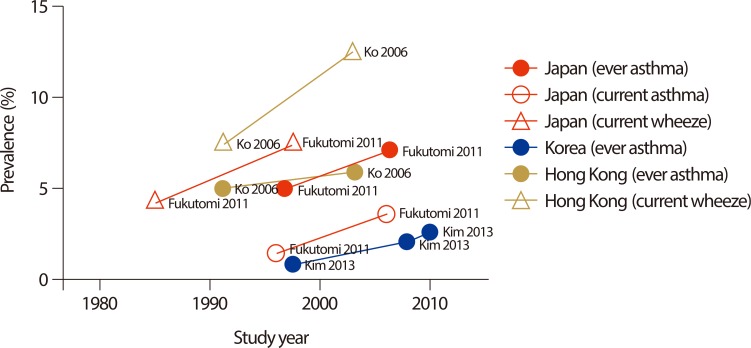
In our review, temporal changes in Asian adult asthma prevalence were identified in three countries (Japan [43], Korea [38, 44], and Hong Kong [45]). Interestingly, the data demonstrated consistent trends for increasing prevalence, in several asthma definitions including ever asthma, current asthma, or current wheeze (Fig. 4). Statistical significance was directly calculated in the 12-year comparison studies from Hong Kong [45]; they found significant increase in current wheeze (7.5% in 1991 vs. 12.1% in 2003; p < 0.01) but borderline significance in ever asthma (5.1% in 1991 vs. 5.8% in 2003; p = 0.065). In a suburban area in Japan, current wheeze (4.2% in 1985 vs. 7.6% in 1999), ever asthma (5.1% in 1999 vs. 6.7% in 2006) and current asthma (1.5% in 1999 vs. 3.4% in 2006) all showed consistent increase over time [43].
It is not certain whether the adult asthma is also increasing in other Asian countries, as no other longitudinal data are currently available; however, considering the rapid urbanization in Asia, the prevalence is expected to increase in various developing countries. Within the same inherent genetic background, living areas have been associated with the risk of childhood asthma [46]. Adult asthma may be carried over from childhood disease, or newly develop by occupational or environmental irritant exposure [47].
Go to :
WHICH QUESTIONS HAVE BEEN ADDRESSED SO FAR?
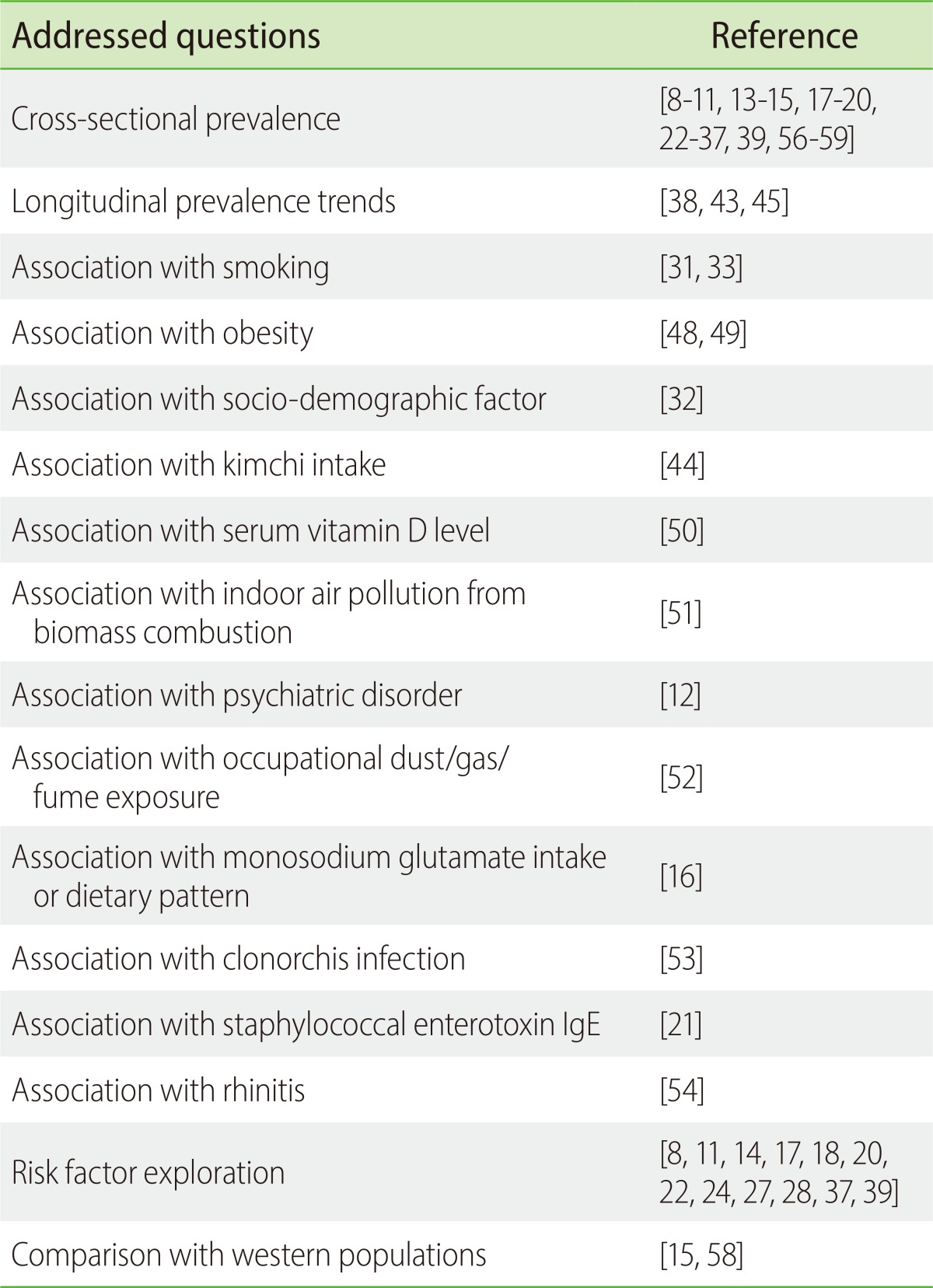
We summarized the research questions addressed in individual studies based on their study purposes (Table 3). Prevalence estimation and risk factor exploration were the most frequent topic. Otherwise, various specific factors were examined in relation to asthma risk, including lifestyle factors (obesity [48, 49] and smoking [31, 33]), dietary or nutritional factors (vitamin D level [50], kimchi [44] or monosodium glutamate intake [16]), pollutant exposure [51, 52], psychiatric disorder [12], clonorchis infection [53], rhinitis [54], or staphylococcal enterotoxin sensitization [21]. These topics of interests have reflected the ideas of Asian researchers, regarding what may underlie the adult asthma.
Go to :
TOWARD A BETTER UNDERSTANDING OF ASTHMA IN ASIANS
Here we summarized the current status of epidemiological research on adult asthma in Asia. Overall prevalence was lower than 5% in Asian adult community populations, which appeared less prevalent than in European adult populations. Importantly, the prevalence of elderly asthma was 1.3-15.3% in Asia, which is relatively high. Because of the population aging due to rising life expectancy and/or declining birth rates in Asia, we have to pay attention to the elderly asthma in this region. However, the methodological heterogeneity was a major limitation hindering the comparison of regional prevalence, despite that the number of conducted studies was not so small in Asia. Temporal trends in prevalence suggested the recent increase of adult asthma in Hong Kong, Japan, and Korea; however, the findings warrant replication in other Asian developing countries.
For these, the utilization of standardized questionnaire tools needs to be encouraged in Asian countries. Although there is no gold standard definition for asthma in epidemiological surveys, at least the academic consensus should be made on the common framework and protocols. The ECRHS and the Global Allergy and Asthma European Network (GA2LEN) projects may be excellent examples to follow. The ECRHS project was initiated for adult respiratory diseases in 1990, consisting of 140,000 participants from 22 countries [7]; currently, the ECRHS phase III follow-up survey is undergoing. The GA2LEN project, consisting of 60 allergy centers from 20 European countries, was a more recent collaboration to integrate European research efforts and capacities for allergy and asthma, and to establish permanent international research network [55]. In each of the projects, the study protocols have been shared in every participating center. In this regard, it may be necessary to prepare for establishing the Asian network for allergy and asthma epidemiological research collaboration. The first workgroup meeting may be held in the next meeting of the Asia Pacific Association of Allergy, Asthma and Clinical Immunology.
Go to :
 XML Download
XML Download