

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Drug hypersensitivity reactions occur at higher rate in human immunodeficiency virus (HIV)-positive patients than general population and cause significant morbidity. Drug hypersensitivity reactions are 100 times more common in HIV patients [1]. In early era of antiretroviral therapy (ART), the incidence of skin rashes can reach 50% of HIV patients taking HIV medications. Diagnosis and management of drug hypersensitivity in HIV-infected patients is difficult because of multiple medication regimens used to treat patients [2]. Hypersensitivity reaction can be caused by antiretroviral agents or antibiotics used to prevent or treat opportunistic infections [1, 2]. It is very challenging to determine which drugs cause the reactions [2].
Go to : 
DRUG HYPERSENTIVITY IN HIV-INFECTED PATIENTS
Drug hypersensitivity is an objective reproducible symptoms or signs initiated by exposure to defined drug at dose tolerated by normal people [3]. It varies in severity and clinical manifestations [4]. Drug hypersensitivity in HIV-infected patients may occur in any type of hypersensitivity classification defined by Gell and Coombs. Clinical manifestations of drug hypersensitivity vary from cutaneous adverse drug reaction (CADR); anaphylactic-like drug reaction; fever; drug-induced hepatic damage; to drug-induced anemia, neutropenia, and thrombocytopenia [5].
Cutaneous eruptions/CADR is the most common manifestation of drug hypersensitivity [4, 6]. Patients can present with exanthema without systemic symptoms or drug hypersensitivity syndromes typically manifesting as an erythematous, maculopapular confluent rash with constitutional features (fever, rigors, myalgias, and arthralgias) in the presence or absence of internal organ involvement (hepatitis, pneumonitis, myocarditis, pericarditis, and nephritis). Stevens Johnson syndrome (SJS) or toxic epidermal necrolysis (TEN) develop in less than 0.5% of patients [4]. A study by Coopman et al. [7] of which included 684 HIV-infected patients from The Harvard Community Health Plan's records showed that CADR accounted for 8.2% dermatologic diagnoses of HIV patients. The most common CADR is morbilliform rash. Others were urticaria, erythema multiforme, vasculitis, exfoliative dermatitis, and photodermatitis [3, 7]. Most of CADR in HIV patients are induced by cotrimoxazole [7]. Antiretroviral medications have also been associated with CADR, ranging from mild exanthemas to life-threatening reactions, such as SJS or TEN [8].
Go to :
PATHOGENESIS
The pathogenesis of drug hypersensitivity is not well defined. Drug hypersensitivity occurs if there is an exposure with a causative agent in a susceptible individual [6]. Genetic predispositions for some of the drugs have been described, especially for abacavir. Abacavir hypersensitivity is strongly associated with the class I major histocompatibility complex (MHC) allele HLA-B*5701 [2]. Evidence showed that there is also involvement of T cells. There are two hypotheses regarding how the drugs presented in vivo: the hapten-dependent and hapten-independent pathways [4, 6]. According to hapten-dependent hypothesis, most drugs become immunogenic through metabolism to reactive intermediates, which can bind covalently or haptenate with proteins. Then they are presented via the human leukocyte antigen (HLA) molecules to T cells. The other hypothesis stated that the parent drug itself could directly activate T cells by interacting with MHC-peptide or T-cell receptor. After stimulation, T-cell infiltrates the skin. CD4 T-cell secrete cytokines such as interleukin (IL) 5, granzyme and eotaxin, which are involved in the recruitment, growth and differentiation of eosinophils. Drug-stimulated T cells can also kill autologous target cells via the perforin pathway. CD8+ T cells are primarily responsible for bullous reactions, but have also involved in abacavir hypersensitivity [4].
Individuals infected with HIV show an increased frequency of drug eruptions when compared with the non-HIV population [6]. The pathophysiology of drug hypersensitivity in HIV is multifactorial and related to changes in drug metabolism, dysregulation of the immune systems (immune hyperactivation, patient cytokine profile), oxidative stress, genetic predisposition, and viral factors [1, 2, 4]. Cutaneous ADRs increased as the immune system deteriorates with the apparent decreasing in CD4+ T-cell count [3, 7]. Other factors related to increase frequency of CADR are increasing age, other associated skin diseases, and evidence of active (acute or reactivation) Epstein-Barr virus and cytomegalovirus infections [3].
Studies showed an increasing immunoglobulin E (IgE) levels in HIV patients of which increase with disease progression and decrease in CD4+ T-cell count. This condition associated with the loss of appropriate host immune response [1]. Compared to HIV negative control, HIV patients have decreased proportion of interferon-γ-producing (Th1 type) CD4+ T-cell clones and increased proportion of IL-4-producing (Th2 type) CD4+ T-cell clones [5]. Immunofluorescence and immunochemistry study from biopsy of HIV patients with CADR showed infiltration of activated CD8 lymphocyte and epidermal production of cytokines [9].
There are also some drug factors that can predispose patients to drug hypersensitivity. This includes large molecular mass, specific immunologic structural moieties, reactive metabolites, parenteral or topical administration, a longer duration of exposure, and frequent, repetitive courses of therapy [2].
Go to :
HYPERSENSITIVITY TO PROPHYLACTIC DRUG
Cotrimoxazole prophylaxis
Cotrimoxazole is the drug of choice for Pneumocystic jirovecii pneumonia prophylaxis as a standard of care in HIV-infected patients with low CD4+ T cell counts. Cochrane meta-analysis showed that cotrimoxazole prophylaxis can prevent death in adults and children with early and advanced HIV disease [10, 11]. Other than prophylaxis for P. jirovecii infection, cotrimoxazole is also used for prophylaxis of toxoplasma encephalitis [12].
The incidence of drug hypersensitivity from cotrimoxazole is higher in HIV patients (40-80%) compared to healthy subjects (3-5%). The risk of CADR from sulfonamide antibiotics is increasing in HIV patients due to immunologic factors and frequent exposure to these antibiotics [4, 8]. Male sex, history of syphilis, CD4:CD8 ratio < 0.10, and low CD4 cell count are related to increase risk of cotrimoxazole hypersensitivity.
CADR is observed mostly 7 days after initiation of therapy. The clinical manifestations vary from urticaria, macular exanthemas, eczematous and fixed drug eruptions, erythema multiforme, SJS, and TEN with associated constitutional symptoms [2, 4]. Chantachaeng et al. [13] revealed that among HIV positive patients, maculopapular rash was the most common cutaneous eruption, followed by SJS, drug hypersensitivity syndrome and fixed drug eruption. These results differ from HIV negative patients in whom the most common manifestation was fixed drug eruption, followed by maculopapular eruption and angioedema with or without urticaria. Low CD4 levels have been proposed to be one of the risk factors for severe CADR because CD8 will subsequently be more dominant [4].
Pathogenesis of cotrimoxazole hypersensitivity is not completely understood. There are probably role of metabolic, toxic, and immunologic factors that can lead to hypersensitivity in predisposed individual [2, 4]. The N4 aromatic amine is critical for the development of delayed reactions to sulfonamide antibiotics [8]. In normal hosts, a small fraction of sulfamethoxazole undergoes oxidation by cytochrome P450 to sulfamethoxazole hydroxylamine. Sulfamethoxazole hydroxylamine is a reactive metabolite and may spontaneously form nitrosulfamethoxazole. This metabolite covalently binds to host proteins, causing direct cellular toxicity. This necrotic cell death may provide a 'danger signal' to sensitized T cells leading to the cascade of immune response and cytokine release. Glutathione deficiency that can decrease inactivation of toxic metabolites can lead patients to higher risk of hypersensitivity [2, 4]. Study by Wang et al. [14] showed that polymorphism in the enzyme involved in glutathione biosynthesis (glutamate cysteine ligase catalytic subunit) is significantly associated with sulfamethoxazole-induced hypersensitivity.
The role of glutathione deficiency lead to a study to use N-acetylsistein to prevent cotrimoxazole hypersensitivity, but a randomized control study failed to show any benefit. In this study involving 238 patients, treatment with N-acetylcysteine 1 hour before each dose of cotrimoxazole could not prevent hypersensitivity reaction [15].
Cutaneus adverse drug reaction caused by cotrimoxazole is usually caused by sulfamethoxazole. Nevertheless, there were some drug rash reports caused by trimethoprim. The manifestations reported were fixed drug eruption, linear fixed drug eruption, and generalized erythematous skin eruptions. The possibility of trimethoprim as the offending drug, highlight the importance of testing trimethoprim and sulfamethoxazole independently [16].
Cotrimoxazole prophylaxis can be continued or readministered after a desensitization protocol in nonimmediate reactions with mild rash and no sign of mucosal or extracutaneous symptom. Cochrane review which included three studies involving 268 adults HIV patients showed that for prophylaxis of opportunistic infections, cotrimoxazole desensitization could result in fewer treatment discontinuations and overall adverse reactions in HIV-infected patients with previous history of mild or moderate hypersensitivity to cotrimoxazole when compared to cotrimoxazole rechallenge [17]. For the treatment of drug reaction with eosinophilia and systemic symptoms (DRESS) with severe organ involvements (e.g., transaminase level more than 500U/L), corticosteroids are often used [18].
Isoniazide preventive therapy
Tuberculosis (TB) remains a common opportunistic infection and a major cause of death among HIV patients, especially in countries where there is high TB prevalence. From The TREAT Asia HIV Observational Database, there were 22% patients diagnosed with TB at baseline. The incidence of TB from this multicenter prospective cohort was 1.98 per 100 person years [19]. The risk is dependent on the degree of immunodeficiency, the socio-economic conditions and the exogenous TB infection [20]. In TB-HIV endemic place, the TB incidence rates remain high although highly active antiretroviral therapy program has already delivered. This fact highlights the need of implementing TB preventive therapy besides enhancing TB diagnosis and screening [21].
Isoniazid preventive therapy (IPT) is one of the strategies to reduce TB infection among HIV patients IPT reduces TB risk by 32% overall and by 64% in the subset of patients with positive tuberculin skin tests and is the key TB preventive intervention prior to ART eligibility [22]. Study by Golub et al. [23] revealed lower TB incidence rates in HIV patients taking antiretroviral (ARV) and IPT compared to ARV alone (1.1 vs. 4.6 per 100 person years).
Hypersensitivity rash is one of the side effects from IPT. A study conducted by Grant et al. [24] involving large number of participants showed that after six months of follow up, 0.25% of patients receiving IPT developed hypersensitivity rash. All rashes were graded as mild to moderate that occur in median of 20 days after IPT start.
Go to :
HYPERSENSITIVITY TO DRUGS TO TREAT OPPORTUNISTIC INFECTIONS
Antituberculosis
Rash and/or fever was the most common serious adverse event in patients treated with antituberculosis (anti-TB) and HIV infection is a risk factor for rash with anti-TB drug [3, 25]. In a prospective study in Nairobi involving 287 adults receiving standard anti-TB drugs, CADRs were seen within the first 16 weeks of treatment in 20% of HIV patients, compared to 1% of HIV-seronegative patients [26]. Another prospective study in children from Zambia found CADR in 21% of children with TB-HIV, compared with only 2% of those who were not HIV [27] The incidence of severe CADR is also higher in HIV patients. A cross-sectional survey conducted in Kenya showed that SJS was reported 4.85 times more common in HIV-positive patients compared with HIV-negative patients [28].
Nonimmediate reactions to anti-TB drugs are more common than immediate reactions. Our retrospective cohort involving HIV patients receiving anti-TB drugs, CADRs occur with median time of 15 days, ranging as fast as 2 days until 3 months. The most common manifestation was maculopapular rash, followed by erythema multiforme, urticaria, angioedema, erythroderma, SJS and TEN [29].
The management of drug hypersensitivity in patients receiving anti-TB drugs is challenging since it is difficult to determine which drug resulted in the hypersensitivity reaction [30]. Drug provocation test, a controlled administration of a drug to diagnose a drug hypersensitivity reaction, can be helpful to know which one is the offending drug [3, 30]. Pattern of anti-TB drug causing drug hypersensitivity reaction varies among many studies. The most common anti-TB drug causing CADR in our study was rifampicin, followed by ethambutol, pyrazinamide, isoniazide, streptomycin, and anti-TB fixed drug combination. A study in Canada showed that pyrazinamide hypersensitivity rash almost double than isoniazide and ethambutol [31]. Almost the same with a report from Malaysia that revealed pyrazinamide was the commonest offending drug, followed by streptomycin, ethambutol, rifampicin, then isoniazide [32].
Antitoxoplasmosis
Toxoplasmic encephatilits is one of the most common central nervous system opportunistic infections in HIV-infected patients [33]. More than 95% of toxoplasmic encephalitis occurs primarily due to reactivation of latent infection. Prevalence of latent Toxoplasma infection in HIV patients in Asia is reported high, up to more than 40% [34]. Other than cerebral manifestation, retinochoroiditis, pneumonia, and other multifocal organ system involvement can be observed after dissemination of infection [12].
The initial drug of choice for treating toxoplasmic encephalitis is the combination of pyrimethamin, sulfadiazine, and leucovorin [12]. Sulfonamides other than sulfadiazines and trisulfapyrimidines are less effective against Toxoplasma gondii [35]. Unfortunately, sulfadiazine is not available in all countries, including Indonesia. The preferred alternative regimen for patients who cannot tolerate sulfadiazine or fail to the regimen is pyrimethamine, clindamycin, and leucovorin. Leucovorin is used to reduce the risk of hematologic toxicities associated with pyrimethamine therapy [12]. There was also a higher incidence of CADR with combination of pyrimethamine and sulfadiazine compared to pyrimethamine and clindamycin (39% vs. 29%) [35]. Another study conducted by Iaccheri et al. [36] in patients receiving antitoxoplasmosis for ocular toxoplasmosis also revealed that rash, accounted for 34.5% of adverse drug reactions, mostly occurred in patients receiving sulfadiazine (22.5%). The mean interval between drug administration and the onset of adverse drug reaction was 14 days (range, 2-45 days).
In our experience, hypersensitivity reaction was commonly observed with the use of pyrimethamine-sulfadoxine tablet (cumulative incidence of 34.2%) before the availability of pyrimethamine tablet. The cumulative incidence of pyrimethamine tablet was found to be decreased to 6.2% among patients using pyrimethamine [37].
Clindamycin hypersensitivity had also been reported, but with lower incidence (0.4-3%) [37, 38]. The manifestations of clindamycin hypersensitivity reported from the literature vary including generalized maculopapular pruritic reaction, angioedema, DRESS, SJS, and TEN [38, 39].
If the patients cannot tolerate sulfadiazine or clindamycin, the alternatives are: cotrimoxazole; atovaquone and pyrimethamine; atovaquone; azithromycin and pyrimethamine; clarithromycin and pyrimethamine; 5-fluorouracil and clindamycin; dapsone and pyrimethamine; and minocycline or doxycycline in combination with either pyrimethamine, sulfadiazine, or clarithromycin [12].
Antifungal drugs
Marked depression of cellular immunity in HIV patients leads to some opportunistic infections including fungal. The most common fungal infection in HIV patients is candidiasis. Other fungal infections include cryptococcosis, histoplasmosis, aspergillosis, dermatophytes, coccoidioidomycosis, blastomycosis, penicilliosis, sporotrichosis, and Pnuemocystic jirovecii infection [40].
Fluconazole is routinely used as consolidation and maintenance therapy for cryptococcal meningoencephalitis and meningoencephalitis caused by coccidioidomycosis. Itraconazole, the other triazole agent, is used for induction treatment of mild histoplasmosis, for maintenance therapy of histoplasmosis, also for treating patients with Penicillium marneffei infection. Newer azoles, voriconazole and posoconazole, may be effective in patients with fluconazole-resistant candida infection. Voriconazole is also effective in treating aspergillosis cases [41].
There were some reports hypersensitivity reactions including maculopapular rash, fixed drug eruptions, diffuse erythema, angioedema, rash with acute hepatitis, and SJS due to fluconazole [42, 43]. In patients with hypersensitivity to fluconazole, itraconazole and voriconazole can be successfully introduced without cross-sensitization occurring [44].
However, itraconazole does not appear to be as effective as fluconazole in the case of cryptococcal meningitis. In this case, fluconazole desensitization might be a choice. Craig et al. [43] reported a successful case of desensitization for fluconazole hypersensitivity. Cytopenias and exfoliative rashes are contraindications for desensitization or rechallenge with fluconazole.
Hypersensitivity to itrazonazole has also been reported. It can occasionally cause a generalized maculopapular rash. Desensitization to itraconazole had been succesfully described in the literature [45]. A report of successful rapid desensitization following posaconazole hypersensitivity has also been described recently [46].
Go to :
ANTIRETROVIRAL DRUG HYPERSENSITIVITY
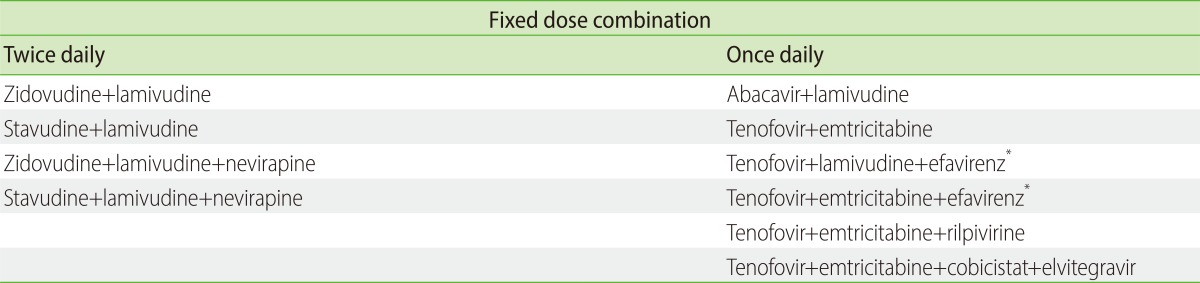
There are 6 classes of antiretroviral drug approved by U.S. Food and Drug Administration based on their mode of actions as shown in Table 1: nucleoside reverse transcriptase inhibitor (NRTI), non-nucleoside reverse transcriptase inhibitor (NNRTI), protease inhibitor (PI), fusion inhibitor, cysteine-cysteine chemokine receptor 5 (CCR5) inhibitor, integrase strand transfer inhibitor (INSTI). Cobisistat, a new drug with no activity against HIV has been introduced as pharmacokinetic (PK) enhancer. PK enhancing is a strategy used in ARV treatment to increase the exposure of an ARV by concomitantly administering a drug that inhibits the specific drug metabolizing enzymes for which the ARV is a substrate. Low dose ritonavir is also classified as PK enhancer [47]. Antiretroviral regimen should consist of at least 3 drugs with different site of action, usually a combination of 2NRTIs with 1NNRTI or 2NRTIs with 1PI. All types of antiretroviral drug can cause adverse drug reactions, particularly drug hypersensitivity. Current World Health Organization guideline recommends once daily fixed dose combination of tenovofir with lamivudine/emtricitabine and efavirenz (Table 2) to simplify the treatment and increase adherence. This regimen is less frequently associated with severe adverse reactions and has a better treatment response compared with other once- or twice-daily regimen [48].
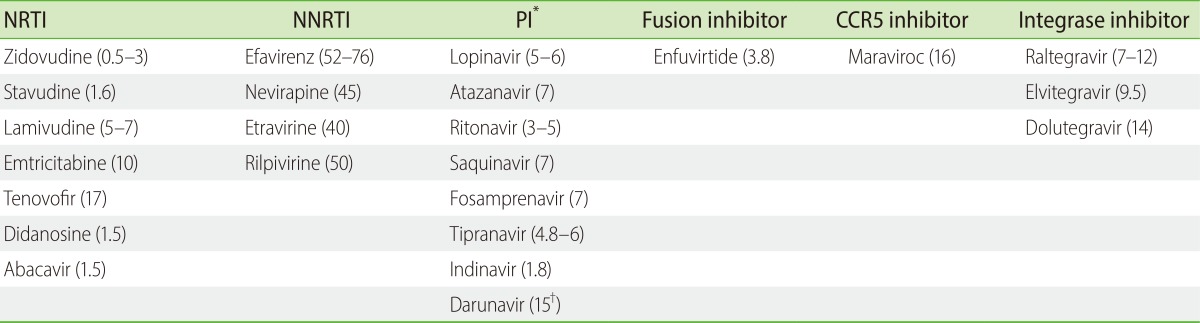
Table 1
Approved antiretroviral drugs to treat human immunodeficiency virus infection and their half-life (in hours)
NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, non-nucleoside reverse transcriptase inhiitor; PI, protease inhibitor; CCR5, cysteine-cysteine chemokine receptor 5.
*Most of PI in combination with low dose ritonavir (100 mg) as boosted PI or pharmacokinetic (PK) enhancer. Other PK enhancer: cobisistat (3.5 hours). †With ritonavir.
![]()
Nucleoside reverse transcriptase inhibitor
Nucleoside reverse transcriptase inhibitors block reverse transcriptase activity by competing with the natural substrate and incorporating into viral DNA to act as chain terminator in the synthesis of proviral DNA [6]. Abacavir is the most well known multiorgan and potentially life-threatening cause of hypersensitivity among antiretroviral drugs in this class. It has been reported to occur in 2.3% to 9% of the patients [49].
Abacavir hypersensitivity reactions manifests as at least two symptoms of fever, skin rash, malaise, nausea, headache, myalgia, chills, diarrhea, vomiting, abdominal pain, dyspnea, arthralgia, and respiratory symptoms. Cutaneous rash, maculopapular or urticarial, only occur in about 70% of abacavir-treated patients. Rash is usually mild and sometimes goes unnoticed by the patient [50]. Of all the cases, 98% of them reported fever or rash or both [51]. The symptoms occur within 5-6 weeks after commencement and resolving within 72 hours of withdrawal of the drug. SJS and TEN are rarely associated with abacavir, but have been reported [52, 53].
If abacavir is stopped due to hypersensitivity, it should never be restarted. Rechallenge with abacavir is absolutely contraindicated. It results in the reappearance of symptoms within hours of re-exposure. Fatal hypotension and anaphylactic-like reactions have occurred in patients who have been rechallenged following a hypersensitivity reaction to abacavir [54].
One randomized, open-label study using prednisolone to prevent abacavir hypersensitivity reaction failed to show its preventive activity. Therefore, this approach never been used in clinical practice [55].
A specific allele of the major histocompatibility complex, HLA-B*5701, has been associated with the development of abacavir hypersensitivity in all the races. With an odds ratio greater than 500, this is one of the most compelling HLA/ADR associations identified ever [56, 57].
Although rare, zidovudine has also been reported as a cause of drug hypersensitivity reaction in early years of antiretroviral monotherapy. The reaction included maculopapular rash, blistering and erythematous lesion, fever, leukocytoclastic vasculitis, and toxic epidermolysis [58, 59].
Tenofovir, a newer NRTI that most commonly used right now, caused maculopapular or vesicular pruritic rash on the face, extremities and trunk in 5-7% of the patients. A photoallergic dermatitis after stavudine substitution to tenofovir and a case of lichenoid eruption with eosinophilia were also reported [60-63].
Non-nucleoside reverse transcriptase inhibitors
Non-nucleoside reverse transcriptase inhibitors bind directly and noncompetitively to the enzyme reverse transcriptase. These drugs block DNA polymerase activity by causing conformational change and disrupting the catalytic site of the enzyme without phosphorylation and incorporating into viral DNA. All drugs on this class are associated with the development of drug hypersensitivity, more common in nevirapine [6].
Nevirapine-associated rash was reported as common as 15% to 32%. The rash is usually maculopapular, occuring in 10 days to 6 weeks of treatment initiation and it is generally mild and self-limited [64, 65]. Rash associated with fever and hepatitis have occurred in approximately 5% of those initiating nevirapine [66]. SJS and TEN have been reported in 0.3-0.37% nevirapine-treated patients in various clinical trials [66, 67]. Discontinuation of nevirapine due to hypersensitivity has been described in 2-10% of HIV-infected patients commencing nevirapine [68].
Severe hypersensitivity and hepatotoxicity events have also been more commonly documented in non-HIV-infected individuals receiving postexposure prophylaxis. Therefore, nevirapine is not recommended to be use for occupational or nonoccupational postexposure prophylaxis [69].
In cases with mild to moderate rashes (erythema, diffuse erythematous macular or maculopapular rash) without constitutional symptom or organ dysfunction, the drug can be continued without interruption. If rash occurs during lead-in period, the dose should not be escalated until rash resolves. If nevirapine has been discontinued for more than 7 days, it should be resumed at 200 mg once daily and escalated after 2 weeks without complication. In cases with severe rashes such as extensive erythematous or maculopapular rash or moist desquamation, angioedema, serum sickness-like reactions, SJS, and TEN, immediate and permanent discontinuation is warranted. We should not continue nevirapine in suspected nevirapine-associated rash with consitutional symptoms like fever, significant liver function test elevation, blistering, oral lesion, conjunctivitis, facial edema, arthralgia, and general malaise, nor in cases with organ dysfunction [70].
Current recommendation of nevirapine dose escalation due to autoinduction of the drug metabolism is 200 mg daily for 2 weeks followed by 200 mg twice daily thereafter. Another option is using a slower escalating dose, a 100 mg daily dose of nevirapine, escalating 100 mg daily per week up to 400 mg daily at the fourth week. A study in 1998 shown that this slower escalation dose provide a lower incidence of rash leading discontinuation of therapy in comparison with the standard initial (2.1% vs. 8.5%) [71].
Efavirenz, the most common NNRTI used in clinical practice, has been associated with rash in 4.6-20% of patients commencing the drug, commonly manifested as mild to moderate rash [72]. The pattern of systemic symptoms and organ involvement, including fever, myalgia, arthralgia, transaminase elevation is almost the same with nevirapine, but rarely occur compared to nevirapine. Severe drug eruptions such as SJS, TEN, and erythema multiforme were reported in 0.1% of patients, compared with 0.3-1% reported with nevirapine [73, 67].
Rashes in patients taking efavirenz usually occur in the second week of therapy (median onset 11 days). If the rash is not severe, treatment with efavirenz can be continued with addition of antihistamines or topical steroids. The rash will usually resolve within 4 weeks [6].
Cross-hypersensitivity between nevirapine and efavirenz had been reported in early study [74, 75]. However, a retrospective study in Thailand demonstrated that the majority (91.8%) of HIV-infected patients with CD4 counts <200 cells/mL who had preceding nevirapine-associated rash could tolerate efavirenz well. Therefore efavirenz might be used as antiretroviral drug substitution in patients who experience nevirapine-associated skin rash, especially in resource-limited settings where options of antiretroviral agents are limited [76]. Nevirapine may also be an optional choice for patients with a history of efavirenz-associated rash [77].
Rash is common side effect of etravirine, the second generation of NNRTI. Most rashes were mild-moderate maculopapular rashes and resolved with etravirine continuation. The rash occur most often during the second week of therapy and leads to drug discontinuation in 2% of patients [78]. Other severe and life-threatening hypersensitivity reaction such as of SJS, TEN and erythema multiforme were also described [79].
Rilpivirine, another new NNRTI rarely cause drug hypersensitivity. In two large, multinational, randomized, double-blind clinical trials comparing rilpivirine with efavirenz, drug discontinuation due to rash were more frequent with efavirenz than with rilpivirine [80].
Protease inhibitors
Protease inhibitors act by inhibiting the HIV-1 protease enzyme, which is responsible for cleavage of the large viral gag and gag-pol polypeptide chains into smaller functional proteins, allowing maturation of the HIV virion. All PIs have been documented to cause drug hypersensitivity syndrome. The estimated rate of hypersensitivity rash in patients treated with a PI was around 5%. There is no allergic cross-reactivity between PIs [6].
Amprenavir is the PI that most frequently produces drug hypersensitivity (28%) while fosamprenavir, a prodrug of amprenavir, has been associated with skin rash in 19% of patients. Amprenavir or fosamprenavir-related rash usually occurs at within 2 weeks from drug initiation and may be accompanied by fever or elevated transaminase. Mild to moderate rashes do not require treatment discontinuation. Treatment discontinuation due to more severe rash was observed in less than 1% of the patients. SJS cases had been described after commencing both amprenavir and fosamprenavir [81]. Amprenavir and fosamprenavir share the same sulfonylarylamine structure with sulfamethoxazole. Eventhough there is limited information about cross hypersensitivity of these PIs with sulfonamide drugs, these medications should be used with caution in patients with known sulfonamide allergy [18].
Lopinavir/ritonavir has been implicated in a wide range of early skin adverse reactions. The rate of maculopapular rash related to lopinavir/ritonavir was estimated to be 2% to 4%. Cases of acute generalized exanthematous pustulosis and multiorgan hypersensitivity reaction due to lopinavir/ritonavir have been reported [4, 6].
Atazanavir has not commonly been associated with the occurrence of a rash, although reported as 6% in the drug trial [4]. To date, only few published cases describing atazanavir-associated rash in the form of macular or maculopapular rash had been reported. In some cases, the rashes were associated with jaundice, elevated liver enzymes, and hyperbilirubinemia [4, 82].
Fusion inhibitor
Enfuvirtide, the only drug in fusion inhibitor class, acts by inhibiting the fusion of HIV-1 with CD4+ T cells. This drug is administered by subcutaneous injection. Hypersensitivity to enfuvirtide is rare, less than 1% of the patients developed systemic hypersensitivity in clinical trial. Combinations of fever, rash, systemic features and hepatitis occur after 1 week of drug initiation [84]. Discontinuation of enfuvirtide was recommended in all cases [4, 84].
CCR5 inhibitor
HIV enters cells by a complex process that involves sequential attachment to the CD4 receptor, followed by binding to either the CCR5 or C-X-C chemokine receptor 4 molecules and fusion of the viral and cellular membranes. CCR5 coreceptor antagonist (maraviroc) prevents HIV entry into target cells by binding to the CCR5 receptors. Therefore, coreceptor tropism assays should be performed whenever the use of a CCR5 antagonist is being considered [47]. Maraviroc hypersensitivity is rare and only reported as part of a syndrome related to hepatotoxicity. Pruritic rash may precede the development of hepatotoxicity. Therefore, patients with signs or symptoms of rash, eosinophilia and elevated IgE should be evaluated to evidence hepatotoxicity [4, 49].
Integrase strand transfer inhibitors
Integrase inhibitors or integrase strand transfer inhibitors act by selectively inhibits the strand transfer activity of HIV-1 and its integration into human DNA [49].
Raltegravir, the first drug in this class is rarely reported as cause of hypersensitivity reactions. The majority of reported rashes was mild to moderate and did not cause drug discontinuation. The rash is tipically maculopapular and generalised [49].
Dolutegravir and elvitegravir are the newer drugs of this class. Elvitegravir is available only as a fixed-dose combination product with cobicistat, tenofovir and emtricitabine [47]. Hypersensitivity reactions to dolutegravir have been also been reported and were characterized by rash, constitutional findings, and sometimes organ dysfunction, including liver injury in less than 1% in clinical trial [85].
Go to :
CHALLENGING MANAGEMENT
Diagnosis and management of drug hypersensitivity is particularly challenging since many patients take multiple drugs and develop opportunistic infections. The last drug introduced might not always be the cause of the reaction because the onset of an allergic reaction is usually delayed, between 1-6 weeks and up to 3 months after commencing the drug. Stopping the drug, especially opportunistic infection drug, may pose the patient to the danger. We might not be able to stop the drug for a long time in preparing drug patch test, especially in patients with low CD4 cell count. To date, success with patch testing in cases of suspected antiretroviral hypersensitivity has only shown in abacavir hypersensitivity. However, abacavir patch testing remains a research tool in clinical trials and not a validated diagnostic test to identify possible abacavir hypersensitivity [86]. HLA-B*5701 screening before starting abacavir has been shown to decrease the incidence of hypersensitivity and routinely used in high-income countries [47, 57]. However, genetic screening for abacavir hypersensitivity would likely be cost-effective in a predominantly white population for whom the prevalence of the HLA-B*5701 allele is 6-8%, but much less cost-effective in Asian/African or African American populations for whom the prevalence are < 1% and 2.5% respectively [87].
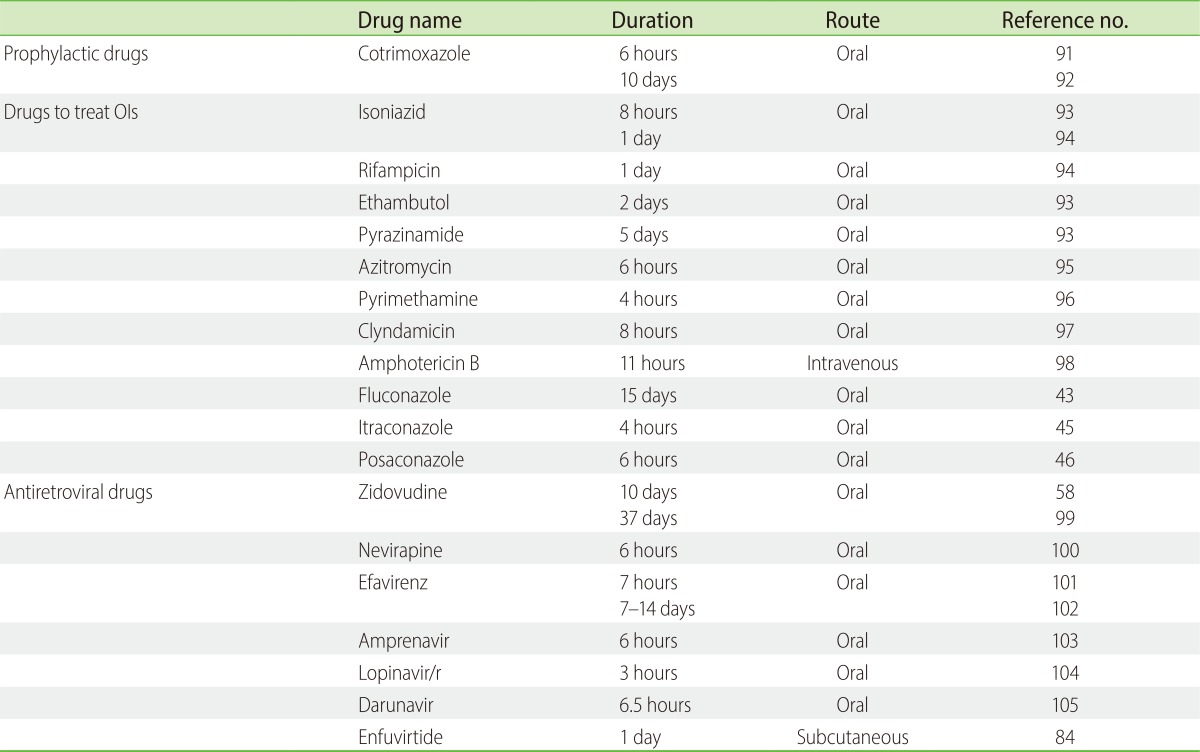
A step wise rechallenge test or desensitization with the offending drug might be preferable action when there is thought to be a clinical need for a particular agent. Stopping and rechallenging the drug should be done under closed supervision. It is also important to note that sometimes patients can be treated through the rash when it is mild to moderate and not accompanied by systemic symptoms and internal organ involvement [2, 4, 6]. However, drug rechallenge is absolutely contraindicated in abacavir hypersensitivity reactions and SJS/TEN [54]. Several successful protocols for drug desensitization are shown in Table 3. Thus, the diagnosis of drug hypersensitivity therefore depends on carefully evaluating the time relationship, the effect of stopping and rechallenging, and exclusion of other possible causes [2].
Stopping antiretroviral drugs with different half-lives might cause drug resistance [47]. Table 1 shows different half-lives of all antiretroviral drugs. The physician should realize when the drug could be continued or need to be terminated and when to restart the same drug or replace with other the drug.
Discontinuing a combination of 2NRTIs and 1 NNRTI, for example zidovudine lamivudine nevirapine, all in the same time may result in functional monotherapy with the nevirapine because NNRTIs have much longer half-lives than NRTIs and other agents. This monotherapy may further increase the risk of NNRTI-resistant mutation and limit future antiretroviral options [47]. The optimal interval between stopping NNRTIs with other antiretroviral drugs is not known. The duration of detectable levels of nevirapine or efavirenz after stopping ranges from 1 week to more than 3 weeks [88, 89]. Many experts recommend stopping NNRTI with the continuation of other antiretroviral drugs for a period of time, in case of nevirapine discontinuation for 4 or 7 days [47]. A study in South Africa revealed that giving 4 or 7 days of zidovudine and lamivudine after single dose of nevirapine reduced the risk of nevirapine resistance from 60% to 10-20% [90]. After rash disappearance during this interval, efavirenz can be introduced directly. However, in severe form of drug hypersensitivity such as TEN when the patients might still be very ill in 7 days, zidovudine and lamivudine might be discontinued until the resolution of TEN. Data on etravirine of rilpivirine treatment interruptions are not available, but their long half-lives suggests that stopping these drugs needs to be done carefully, probably using the same suggestions for nevirapine and efavirenz discontinuation [47].
Clinicians should avoid discontinuing agents with anti-HBV activity in patients with hepatitis B coinfection. Stopping tenofovir, lamivudine, emtricitabine in this population may cause hepatic failure due to reactivation of HBV. However, if discontinuation is unavoidable, patients should be carefully monitored during HBV drug interruptions [47].
The management of these reactions will become even more challenging as different antiretroviral agents are formulated in 1 pill for the ease of patient administration as shown in Table 2. Some patients develop drug hypersensitivity reactions when using fixed drug combination tablet, but not with all of the containing drugs, as observed in our study of anti-TB drugs [29].
Go to :
 XML Download
XML Download