

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Allergy is one of the most common diseases medical practitioners face, with allergic rhinitis (AR) bearing a health burden of 10 to 20% of the global population [1-3]. Being multisystemic in nature, allergy has variable clinical presentations including AR, asthma and eczema, with individualized impact on patients. To alleviate the symptoms of allergy which plague many in the population, there is a significant need to prioritize achieving good clinical practice in the management of patients with allergic diseases.
Using the opportunity of the 1st International Basic Allergy Course (2010), this study identifies and analyses frequently-asked questions by healthcare workers involved in allergy practice, coming from diverse backgrounds in the Association of Southeast Asian Nations (ASEAN) region. Following the 1st International Basic Allergy Course in 2010, similar questions were raised consistently throughout the subsequent courses conducted over the next 3 years. These questions are a good reflection of the common questions in allergy practice, and remain relevant today. An analysis of the collated questions points to a need for an improvement in the dissemination of international guidelines and consensus statements which have been developed to provide clinicians with basic recommendations for the diagnosis and management of AR.
Go to : 
MATERIALS AND METHODS
Course information
The 1st International Basic Allergy Course (2010) was a 3-day course held in Singapore which focused on basic knowledge of allergy, including pathophysiology, diagnostic approach and management. This course was jointly organized by the American Academy of Otolaryngic Allergy Society and ASEAN Rhinological Society. Other topics discussed included asthma, food allergy and the future of allergic practice. Practicum sessions on skin prick testing were also conducted for participants to gain first-hand experience. Similar courses were held in the subsequent years, namely the International Advanced Allergy Course (2011) and the Singapore Allergy & Rhinology Course in 2012 and 2013.
The 1st International Basic Allergy Course was open to all healthcare professionals. There were 268 participants, 143 males and 125 females, comprising 106 Ear, Nose and Throat (ENT) specialists, 87 general practitioners, 34 ENT trainees, 13 nurses, 10 medical students, 2 pharmacists and 16 physicians of various specialties from a total of 16 countries, where most of them were from the ASEAN countries.
Collation of questions
Question and answer sessions were held after every lecture to allow participants to raise any queries. Seven medical students who attended the 3-day course took down all questions raised. In addition, the entire course was video recorded to ensure accuracy of transcription.
The questions were classified into various categories after careful paraphrasing, and care was taken not to alter the context of each question. The team then made reference to the 2001 and 2008 Allergic Rhinitis and Its Impact on Asthma (ARIA) documents [1, 2] for answers to the questions. Further analysis of the questions was carried out to analyze probable reasons for information gaps as well as identify areas for improvement.
Go to :
RESULTS
A total of 103 questions were recorded from the course and divided into eight categories. Fig. 1 shows the distribution of the questions in each of the eight groups. The full list of categorized questions can be found in Supplement.
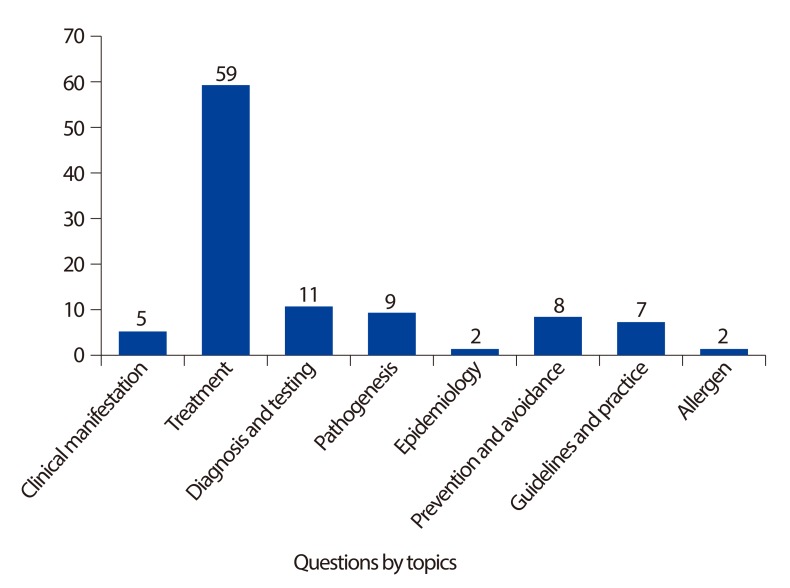
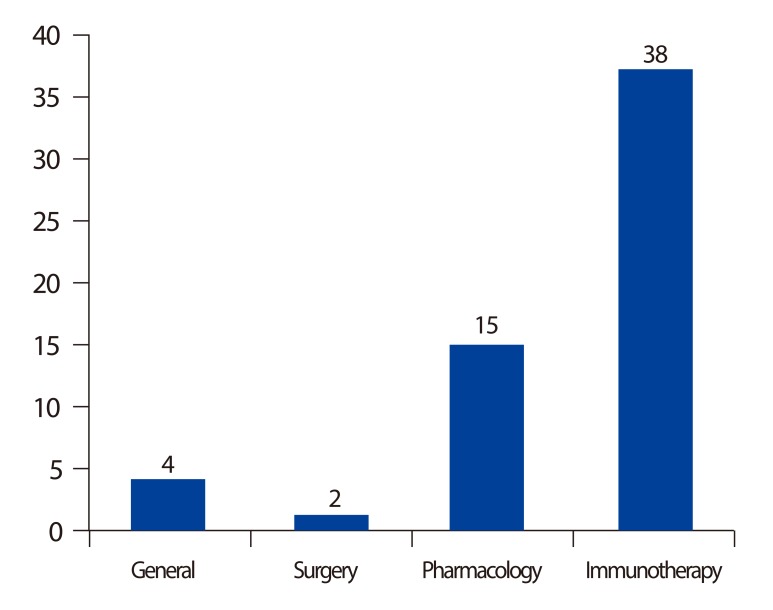
The most frequently asked questions were with respect to treatment in allergy practice (n = 59, 57.3%) (Fig. 2). Of the 59 questions that were asked regarding treatment modalities in allergy practice, 38 were regarding immunotherapy, 15 were related to pharmacologics, 2 were related to surgery, and 4 were general questions. As most questions were on immunotherapy, we subcategorized them into methodology (n = 15), patient selection and indications (n = 10), complications of immunotherapy (n = 8) and evaluation of immunotherapy (n = 5). In the category of "patient selection and indications" (n = 10), 3 were regarding age criteria for starting immunotherapy, 1 regarding symptoms and severity, 5 regarding the usage of sublingual immunotherapy (SLIT) for different allergic conditions and 1 regarding the affordability of SLIT.
41 questions (39.8%) have answers based in the ARIA guidelines [1, 2]. Certain questions were selected for further analysis because they appeared to be a) more commonly asked or b) were deemed to be challenging, even controversial, as the recommendations in current international guidelines were less well-defined.
Questions with regards to the definition of various terms used in allergic practice were frequently raised, such as the differences between 1) "food intolerance", "food allergy" and food hypersensitivity", and 2) vasovagal reactions and anaphylactic/anaphylactoid reactions. As clear definition of terms would enable effective and clear communication among all healthcare workers, this paper would also be exploring these areas.
Go to :
DISCUSSION
Management of allergy requires efforts from a multidisciplinary team. Although international guidelines or consensus documents have been introduced by various professional organizations in the past 10-20 years, dissemination can still be improved, especially amongst primary care physicians, who are often the first point of contact and the main providers of care to the majority of patients with allergic conditions. We have recently reported discrepancies and a lack of public education programs for AR prevention and management in Asia-Pacific countries/regions [4]. For example, there are controversies in recommended minimum age, doses and potential side-effects of many commonly used second-generation antihistamines and intranasal corticosteroids [4]. In this study, several key recurrent themes surfaced from our analysis of the questions collated.
Frequently asked questions
Out of the 103 questions posed during the 3-day course, only 9 were related to "pathogenesis" and 2 on "epidemiology". This does not reflect the true nature of the amount of evidence-based literature in these areas to date. This could possibly be due to the demographics of the course participants, who are mainly clinicians from the ASEAN region. There may be greater interest in topics pertaining to clinical applications and management options as opposed to academic curiosity about epidemiology and pathogenesis of allergy. More research should be carried out regionally to identify disease patterns in our geographical area and uncover any differences in disease presentation and trends as compared to Europe and the United States. This can potentially enable us to develop better management strategies to cater to patients with allergic diseases in our population.
As mentioned, 41 out of 103 questions posed during the course could be answered with information found from the ARIA guidelines [1, 2]. Many of the remaining questions can be addressed by allergy books and guidelines from other international or national bodies. This begs the question as to why lack of familiarity with the guidelines in medical practitioners persists despite easy accessibility of the ARIA guidelines. Our team puts forth certain possibilities for the situation. Firstly, we postulate that doctors may be unaware of the presence of the ARIA guidelines. Secondly, the lack of time coupled with the length of the guidelines may hinder doctors from reading them in spite of their awareness of its availability.
The ARIA guidelines are available in full version and a consolidated pocket guide form [5]. They are written for healthcare professionals like ENT specialists, general practitioners and pharmacists. As such, it can be difficult for the layperson to understand the guidelines. Therefore, more can be done to ensure the dissemination of the ARIA guidelines to members of the public apart from the healthcare fraternity. This can be achieved by publishing guidelines targeted at the laymen, with minimal medical jargon and prior medical knowledge required. We also propose that guidelines be revised to contain specific management recommendations pitched at the level of different healthcare staff in the multidisciplinary team involved in the care of the allergic patients (e.g. general practitioner, pharmacist, advanced practice nurse, ENT specialist).
Sixty-two questions (60.2%) could not be answered by information provided in the ARIA guidelines [1, 2] or the expert panel of speakers during the course. This could possibly be due to lack of evidence-based data such that the ARIA taskforce is unable to adequately provide recommendations to the masses regarding these queries. For example, it remains controversial as to when the efficacy of immunotherapy should be evaluated (from time of commencement) to distinguish between responders and non-responders to immunotherapy. More research could be done in terms of evaluating the different treatment modalities as well as developing specific step-wise algorithms for the initiation of immunotherapy. This would encourage and guide physicians who may be deterred from using such treatment due to the lack of formalized guidelines.
Food intolerance, food allergy and food hypersensitivity
Food intolerance, food allergy and food hypersensitivity are terms that have similar definitions and are often used interchangeably. Difficulties arise when diagnosing and assessing non-IgE mediated reactions to food, and this remains an area of great controversy even among highly regarded specialists in this field. General allergists in the United States [6], however, tend to use the term food sensitivity, which appears to be synonymous with food hypersensitivity used by their European counterparts [6, 7]. Food hypersensitivity, on the other hand, appears to be used to describe non-IgE food allergy. Hence, food allergy only encompasses IgE-mediated allergic reactions, compared to all immune-mediated allergic reactions as defined by EAACI [7].
The terminology that appears to have gained credibility [8] among healthcare providers is that adopted by the European Academy of Allergology and Clinical Immunology (EAACI) (Fig. 3) [7]. The EAACI classifies adverse food reactions, which are divided into toxic and non-toxic reactions. Toxic food reactions are a result of direct action of food components with no involvement of immune mechanisms. Examples of such toxic food reactions are contaminants in food. Non-toxic food reactions can be further classified into immune-mediated or non-immune-mediated reactions.
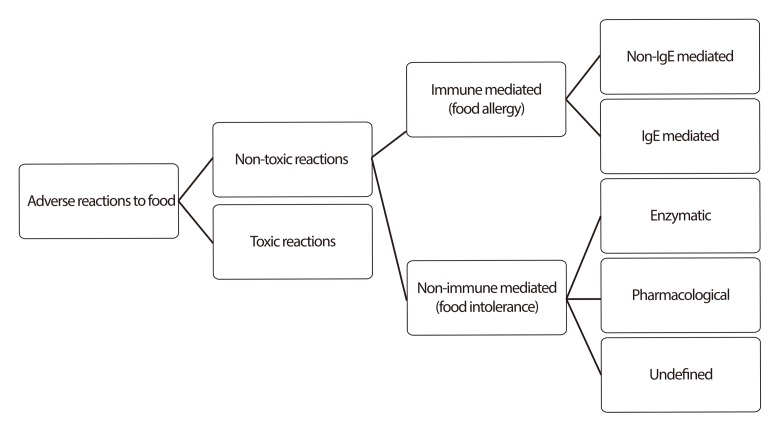 | Fig. 3Types of adverse reactions to food as classified by European Academy of Allergology and Clinical Immunology [7].
|
Immune-mediated food allergy can be subdivided into two categories, IgE mediated and non-IgE mediated food allergy [7]. While the fundamental mechanism of IgE-mediated food allergy is rather well established, the same cannot be said for non-IgE-mediated food allergies. Non-immune mediated food allergy can also be called food intolerance, and can be divided into enzymatic, pharmacological and undefined food intolerance. An example of enzymatic food intolerance is lactose intolerance caused by lactase deficiency. Individuals may develop food intolerance to vasoactive amines like histamines, serotonin and tyramine, known as pharmacological food intolerance. Any reproducible adverse reaction to food due to an unknown mechanism can be classified as food intolerance.
Vasovagal reaction and anaphylaxis/anaphylactoid reaction
Vasovagal reaction and anaphylaxis often present similarly, but have vastly different prognoses. Anaphylaxis is a life-threatening generalized or multisystemic hypersensitivity reaction [8], triggered by exposure to antigens. Immediate treatment is imperative as mortality rate approaches 10% in anaphylactic shock [9]. Vasovagal reactions, following painful interventions such as injection, are commonly confused with anaphylactic reactions. Given the severity of the latter, it is of paramount importance that health professionals are able to differentiate between the two reactions without delay.
Signs and symptoms observed in vasovagal or anaphylactic reactions can be classified according to systems: cardiovascular, respiratory, skin, central nervous system and genitourinary (Table 1) [6, 10]. In anaphylactic reactions, the organs richest in mast cells are primarily affected - respiratory tract, blood vessels and skin. Unsurprisingly, the differences between the two reactions in these three systems are also most pronounced.
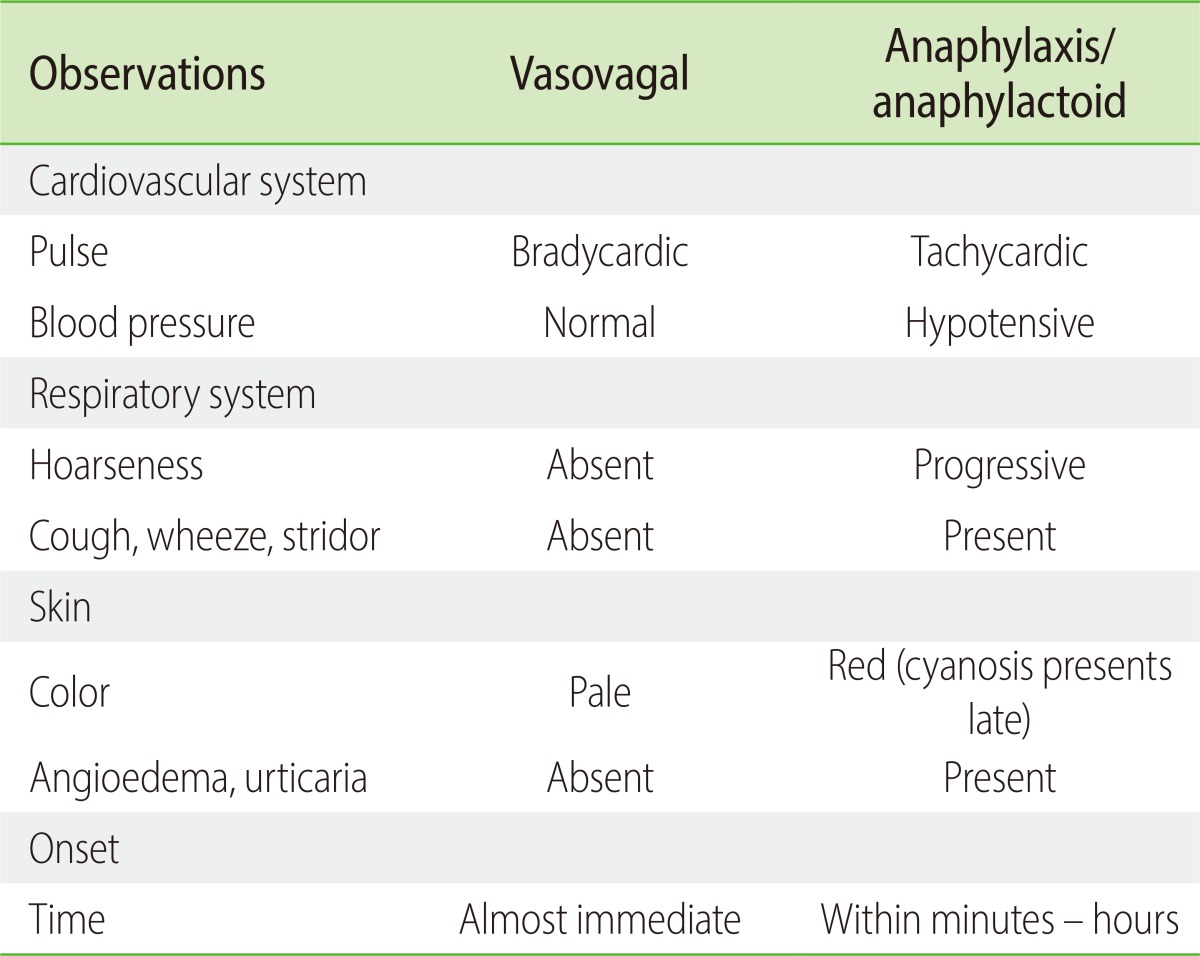
In anaphylactic reactions, the patient would be hypotensive and tachycardic, with a weak or absent central pulse. He/she would have generally flushed, warm skin; little perspiration, and may be cyanotic late in the episode. Contrastingly, if the patient were experiencing a vasovagal episode, he/she would have a slow pulse rate with a strong central pulse. Blood pressure could be low to normal; hypotension should be only transient and would be corrected in the supine position. Pale and cool skin with generalized pallor and profuse perspiration may be observed. Angioedema, urticaria, conjunctivitis and rhinitis seen in anaphylactic patients would be absent in patients with vasovagal reactions.
Patients experiencing an anaphylactic reaction may present with itchy mucous membranes of the respiratory tract, increased nasal secretions or congestion, and progressive hoarseness of voice. They may be coughing, wheezing and dyspnoeic. Patients could also experience nausea, diarrhea, abdominal pain, urinary urgency and uterine cramps late in the anaphylactic episode. On the other hand, patients with vasovagal reactions would not experience any changes in their respiratory tracts, genitourinary or gastrointestinal systems. The loss of consciousness in patients with a vasovagal episode would be transient, and they may be anxious during the consultation. On the contrary, patients with anaphylactic episodes would lose consciousness only later, and they would have a feeling of impending doom. It is also important to note that the onset of vasovagal reactions is almost immediate, within minutes of inoculation, while it may occur in minutes to hours in the case of anaphylactic reactions.
In conclusion, our study identified several problems that if tackled, could help minimize confusion and provide better care for patients suffering from allergic diseases. Also, to leverage on the multidisciplinary approach to allergy, it is important to pitch recommendation guidelines at the level that different healthcare workers involved in allergy management are able to provide. Deeper research into the emerging areas in allergy management such as immunotherapy should be done so that physicians are provided with clearer guidelines and algorithms to start treatment in their patients confidently, and troubleshoot potential problems in the process.
Go to :
 XML Download
XML Download