

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Radiocontrast media (RCM) is a major cause of drug hypersensitivity reactions as the application of RCM is increasing recently in medicine [1]. Although the incidence of RCM induced hypersensitivity reactions was decreased after high-osmolar contrast agents were replaced by low/iso-osmolar agents, increasing number of diagnostic tests using RCM such as computed tomography makes the hypersensitivity to RCM a big issue [2]. RCM induced hypersensitivity reactions are still considered as unpredictable type B hypersensitivity reactions. Underlying mechanism of RCM induced hypersensitivity was previously regarded as nonimmunological mechanisms but recent evidences suggest that immunological mechanisms could also be involved [3, 4, 5]. As a result, the roles of skin tests and premedication are revisiting. In the Asia Pacific region, several studies on RCM induced hypersensitivity reactions have been published including the prevalence clinical manifestations, diagnostic tests and preventions [4, 6, 7]. However, there has been no report that comprehensively summarized and analyzed the results of the studies on RCM hypersensitivity in the Asia Pacific region.
In this article, we aimed to review the literatures semisystematically on hypersensitivity reactions to RCM in terms of prevalence clinical manifestations, diagnostic approach, and prevention in the Asia Pacific region. Two independent authors searched literatures from MEDLINE, Embase, and KoreaMed to identify relevant publications on RCM hypersensitivity from the Asia Pacific region. Searches were limited to articles published in English or Korean, human studies. Search terms included MeSH headings and text words; (contrast media or contrast), combined with (hypersensitivity, allergic reaction, anaphylaxis).
THE PREVALENCE OF HYPERSENSITIVITY INDUCED BY RCM
The prevalence of hypersensitivity reactions showed a difference according to the type of RCM and the onset of the reactions (Tables 1, 2). Immediate reactions that occur within an hour after exposure are nonimmunological or immunoglobulin E (IgE)-mediated reactions while delayed reactions, which occur from an hour to 7 days after exposure, are suggested to be type 4 hypersensitivity reactions that mainly mediated by T cells.
There were several studies on the prevalence of the immediate reactions from Korea (3), Japan (3), Australia (1), India (1), Thailand (1), Turkey (1), and Qatar (1) since 1988. The overall prevalence of immediate reactions was 6.4-31.2% with ionic RCM and 0.16-7.7% with nonionic RCM. In 21st century, the overall prevalence was 0.16-2.21% from the studies.
In case of delayed type hypersensitivity reactions, there were studies from Japan (5), Korea (2), Thailand (1), and Turkey (1) since 1982. The overall prevalence was 0.03-16.5% since 1982 in the Asia Pacific region. The overall prevalence was 0.03-1.95% in 21st century.
CLINICAL MANIFESTATIONS AND RISK FACTORS
Immediate reactions are cutaneous (itching and urticaria), respiratory (bronchospasm and dyspnea), or cardiovascular (dizziness and anaphylactic shock). Delayed reactions are usually cutaneous symptoms such as itching, maculopapular exanthema, Stevens-Johnson syndrome, and toxic epidermal necrolysis [2].
Severe reactions
Although the prevalence of severe reactions varied depending on the studies, severe life-threatening reactions was 0.04-0.28% [1, 2, 4, 6, 7, 8, 9]. It has also been reported that RCM was the most responsible drug that accounted for 18.0% of in-hospital anaphylaxis in a Korean study conducted in a tertiary hospital [1].
Onset of reactions
In a large-scale research in 1990, 70% of RCM hypersensitivity reactions occurred within 5 minutes after injection of RCM agents [10]. Another study, which used only iomeprol, reported that 46.4% of reactions were shown within 10 minutes after injection [11]. However, RCM induced anaphylaxis can also occur hours after the exposure [2].
Risk factors: gender
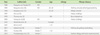
Previous studies reported no significant difference between genders in RCM hypersensitivity reactions [9, 10, 11]. Interestingly, a recent study conducted in Turkey (1,131 subjects), in Australia (29,962 subjects), and Thailand (55,286 subjects) showed that female gender was one of significant risk factors in RCM-induced hypersensitivity reactions [12] (Table 3).
Risk factors: age
A recent Korean study showed that subjects over 50 years old showed statically significant higher incidence of hypersensitivity (p = 0.037) [7] (Table 3).
However, a Japanese study published in 1990 showed that overall RCM hypersensitivity reactions were most common in the age of 20-29, especially severe in 10 to 19 years old [10]. An Australian study showed that patients under 55 years old had significant risk of the RCM hypersensitivity reactions (odds ratio, 2.46; p = 0.005) [13].
RCM hypersensitivity reactions induced by high-osmolar ionic RCM did not show any difference according to age in Indian population [9].
Risk factors: the types of procedures
In a study from Korea [2], computed tomography (CT) was the most common procedure (3.9%) that caused RCM hypersensitivity, followed by angiography (1.1%), magnetic resonance imaging (MRI) (0.8%), and fluoroscopy (0.2%). One case of anaphylaxis occurred during CT angiography.
The use of MRI dye may be safe; however, it can possibly induce anaphylaxis [14]. Thus, physicians should be aware that hypersensitivity reactions can also be caused by MRI dye. In a study from Korea, among the 112 hypersensitivity reactions caused by MRI contrast media, urticaria was the most common symptom observed with 102 cases (91.1%). In addition, respiratory symptoms occurred in 17 cases (15.2%); hypotension in 11 cases including one fatal case (9.8%); angioedema in six cases (5.4%) and other multiple symptoms in 19 cases (17.0%) [14].
Risk factors: allergy
Previous history of allergy could increase the risk of hypersensitivity reactions to RCM [10, 11, 15, 16]. Asthma could be related with more severe reactions (Table 3).
In a study in 1988, a group with history of allergy, asthma, urticarial, or other hypersensitivity showed 52% rate of hypersensitivity reactions compared to patients without the allergy history (7.1%) [17]. Especially, asthma has been reported as a risk factor of severe reactions. In another large scaled study [10], asthma had higher incidence of severe RCM hypersensitivity reaction compare to other allergy such as atopy, pollinosis, drug allergy, and food allergy. Similarly, recent study in Thailand [16] presented that although a history of seafood allergy increased overall incidence of RCM hypersensitivity, and that patients with asthma history has more severe reactions.
DELAYED REACTIONS
Delayed reactions to RCM are relatively difficult to be noticed because they may appear few days after injection and could be confused with symptoms induced by other factors. In one study [18], the prevalence of delayed reaction was 12.4% and none of the risk factors, such as patient's gender, age, history of allergy, were related with the prevalence of delayed reaction. The other study suggested female who were over the age of 40 was at risk of drug eruption by nonionic RCM [19]. Since CT exam is performed more often in older patients, 74.1% of all patients were older than 40 years old.
Among 11,121 patients who responded to the questionnaire in a Japanese research [20], 9.5% showed delayed reactions. There were four risk factors of delayed reactions which include no previous history of examinations using contrast media; past adverse reactions caused by contrast media; a history of allergy and a serum creatinine level greater than 2.0 mg/dL.
DIAGNOSTIC APPROACHES FOR RCM HYPERSENSITIVITY
History taking and physical examination is the main stream in the diagnostic approach. The temporal relationship between the exposure to RCM and the onset of clinical symptom is essential. However, the data for internationally validated laboratory test to detect RCM hypersensitivity has been lacking.
Before current skin test method was widely used [4, 5], researchers tried to predict RCM induced hypersensitivity reactions by injecting a small amount of RCM intravenously before the formal injection [17]. In this study, 48% of pretest positive patients showed hypersensitivity reactions compared to 7.4% of pretest negative group showed only 7.4%. This strong indicator of increased risk of RCM hypersensitivity reaction was not associated with previous RCM exposure history. In an article published in 1991 [22], the characteristics of severe reactions by RCM were evaluated. The value of pretest (injection of small amount of RCM before the procedure) was not sufficient in both ionic and nonionic contrast media, and therefore, the pretest could not predict the risk of severe reaction.
In era of low/iso-osmolar RCM, a study reported that only two among 14 patients with a history of immediate RCM hypersensitivity showed positive skin test in 2011 [16]. Limiting all of the previous reactions to low grade (grade 1 or 2) might have caused low positive rate.
A Korean study was performed to validate the efficacy of RCM skin test to screen RCM hypersensitivity before the administration of RCMs [4]. After 1,048 prescreening skin test, only one showed immediate skin test response (0.09%). Five percent of patients with negative skin test who underwent computed tomography showed immediate reactions. This result suggested that RCM skin test did not have a clinical utility as a screening tool. However, interestingly, the positivity rate of RCM skin test increased as the severity of hypersensitivity reaction higher in patients with RCM hypersensitivity reactions (12.9% in grade I, 25.0% in grade II, 57.1% in grade III). Therefore, the skin test could be useful to identify the causative RCMs in severe hypersensitivity reactions.
Basophil activation test (BAT) could be used as a complementary tool to diagnose RCM hypersensitivity. BAT is a flow cytometry-based cellular assay that measures the activation of basophils upon allergen stimulation using CD63 or CD203c which may detect IgE or non-IgE mediated RCM hypersensitivity [3]. However, the diagnostic value of BAT had not been fully identified. One study performed in Thailand [23], the value of BAT in immediate RCM hypersensitivity was evaluated, and authors identified the activated basophil percentage was significantly higher in patients with previous history of immediate reaction induced by RCM compared with control group. Recently a review article on the value of BAT on RCM hypersensitivity suggested that the sensitivity was 46.2-61.5% and specificity 88.4-100% and that further studies were necessary [3].
Delayed reactions by RCM are usually diagnosed using patch test and delayed reading of intradermal test. The result of those tests in 10 patients with a history of delayed RCM hypersensitivity [16] showed the positive rate of patch test and intradermal test was 10% respectively, but there was no correlation between them.
PREVENTION OF THE RECURRENCE OF RCM HYPERSENSITIVITY
Previous studies had questioned about the usefulness of premedication in RCM. In a large-scale study published in 1990 [10], the relation between hypersensitivity reactions and premedication was evaluated according to the history of allergy and ionic/nonionic RCM. As a result, the positive effect of premedication was shown only in severe hypersensitivity reactions with the ionic contrast media and premedication could not reduce the risk of hypersensitivity reactions in nonionic contrast media group. The effect of premedication in subjects with a history of severe reaction and a positive pretest was analyzed [22], and it also showed no beneficial effect on the prevention of hypersensitivity reactions. In India, patients with allergic diathesis were pretreated with medication such as hydrocortisone, promethazine, theophylline before they were administered with high-osmolar contrast media [9], however, the premedication did not show a prior effect on reduction of hypersensitivity reactions. A case report published in Australia also took the effect of premedication on RCM hypersensitivity pessimistically [24]. Prednisolone 25 mg, cetirizine 10 mg, and ranitidine 150 mg were injected to patients who were diagnosed with RCM-induced anaphylaxis before readministration, but anaphylactic reaction with hypotension recurred even after premedication.
However, recent studies in Korea showed positive outcomes. Thirty patients who had showed immediate hypersensitivity after RCM injection received premedication of prednisolone 50 mg and antihistamine before readministration, and 25 of them didn't have any symptoms after premedication [25]. The success rate of premedication was higher in previous severe hypersensitivity group than mild group (92.3% vs. 76.5%, p < 0.001). Another Korean study [6] compared premedication use and outcome before and after the initiation of a mandatory RCM hypersensitivity reporting and automatic prescription system: intensive premedication with corticosteroid was significantly increased (65% vs. 14%, p < 0.001), and it significantly reduced breakthrough reactions (6.7% vs. 15.2%, p < 0.001).
In 2011, Korean guideline for the safe use of RCM was published by Korean Academy of Asthma, Allergy and Clinical Immunology and the Korean Society of Radiology (Korean Network of Allergists & Radiologists for Research of Radio-contrast Media-associated Adverse Reactions, KOAR3A. In this guideline, if a patient has previous history of severe immediate type RCM hypersensitivity, the preventive measure is 50 mg of oral prednisolone at 13 hours, 7 hours and an hour before injection of RCM, and 4 mg of chlorpheniramine at an hour before the injection. In emergency situations, 40 mg of intravenous methylprednisolone is injected every 4 hours before RCM exposure [26].
CONCLUSION
The overall prevalence of RCM hypersensitivity reactions in the Asia Pacific regions seems to be similar to those in other continents. Immediate reactions (less than an hour after the exposure), delayed reactions (after an hour to 7 days), and severe life threatening reactions (0.04-0.28%) are possible reactions. Type of procedures, allergy and other risk factors could play a role as risk factors. Role of skin test in RCM hypersensitivity revisited especially in the evaluation of patients with severe reactions. However, the value as a prescreening tool is still questionable. Avoidance and looking for alternatives are the best way in a patient with RCM hypersensitivity. Premedication could be helpful when it is necessary and not contraindicated, but physicians should be aware of breakthrough reactions.


 XML Download
XML Download