

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hypersensitivity reactions to betalactams are a frequent cause for allergy consultations worldwide [1, 2, 3, 4, 5, 6]. Patients labeled as allergic to betalactams are more likely to be treated with broad spectrum antibiotics such as vancomycin or quinolones [6, 7, 8, 9, 10, 11] leading to the development of bacterial resistances [12, 13, 14, 15] and subsequent increase in health expenditure [1, 9, 15].
Most reactions to penicillin are skin related and earlier data showed that rates of skin reactions among inpatients are 5.1% with amoxicillin, 4.5% with ampicillin and 1.6% with penicillin [1]. However, anaphylactic reactions were the initial presentation in 0.015% to 0.04% of treated patients [1]. Prevalence of self-reported allergy to penicillin is approximately 5-10% when considering different populations worldwide [1, 3, 4] but, interestingly, 85% to 90% of them have negative skin tests to penicillin when tested [2, 5, 6]. A penicillin skin test predicts only the presence of immunoglobulin E (IgE) antibodies and does not predict non-IgE-mediated reactions caused by other immune mechanisms, such as cytotoxic antibody, antibody-antigen immune complex, and delayed-type cell mediated reactions [1]. Patients with positive history and a positive skin test to penicillin have 50% or greater chance of an immediate IgE-mediated reaction if penicillin is received again [16]. Diagnosis of penicillin allergy cannot rely solely on clinical history. Drug provocation test (DPT) in an appropriate health care facility may assure the safety of readministering the drug [1, 17].
Penicillin is a low molecular weight molecule that splits under physiological conditions to a number of products that can covalently bind tissue and serum proteins leading to formation of new hapten-protein structures that may induce production of specific IgE responses. The core betalactam ring is the principal immunogenic structure and approximately 95% of its products include the penicilloyl group, which is called major determinant (benzylpenicilloyl poly-L-lysine, PPL) the remaining products are called minor determinant mixture (MDM) [18, 19, 20]. Some patients can also develop IgE responses against the side chains of betalactams instead of the main core structure products [21, 22, 23].
The aim of this descriptive study is to analyse the patterns of hypersensitivity to penicillin over a long period of time in Kuwait. We analyse our cohort in terms of demographics, culprit drug, in vivo and in vitro allergic evaluation during a 6-year study period. To our knowledge, this is the first study on the patterns of penicillin hypersensitivity in an Arabian Gulf Country.
MATERIALS AND METHODS
Al-Rashed Allergy Center is a tertiary public allergy center in the state of Kuwait. Drug allergy cases from all hospitals in Kuwait are referred to our center. We conducted a retrospective, descriptive study looking at medical records from all cases of penicillin allergy to Al-Rashed Allergy Center, between 2007 and 2012. Data related to demographics, type of drug, and drug allergy outcomes, were evaluated.
We describe a cohort of 124 patients who were referred for penicillin allergy evaluation. All patients had a history compatible with IgE mediated reactions within 24 hours of drug administration. Patients were excluded if they presented with bullous exanthems, DRESS, Stevens-Johnson syndrome, acute generalized exanthematous pustulosis and toxic epidermal necrolysis [24], or had a history of immediate (<2 hours) anaphylaxis [25].
Skin prick test (SPT) and intradermal testing (IDT) was performed with major determinants undiluted (PPL) (Diater, Madrid, Spain), minor determinants undiluted (MDM) (Diater), Penicillin G 10,000 U/mL (Sandoz GmbH, Kundl, Astria), Ampicillin (25 mg/mL) (Ampicillin Sodium equivalent to 500 mg Ampicillin activity; Bristol-Myers Squibb Co., New York, NY, USA), Amoxicillin (25 mg/mL) (Hymox Forte in powder form; Biocheme Spimaco, Kingdom of Saudi Arabia). Histamine phosphate (10 mg/mL) and saline solution were used as positive and negative controls, respectively. Radioallergosorbent test (RAST) system was used to test total IgE and penicillin specific IgE antibody. DPT was performed regardless the culprit betalactam with phenoxymethyl-penicillin as potassium salt 300 mg (Ospen, Biocheme Spimaco, Kingdom of Saudi Arabia).
Patients were instructed to withhold from systemic antihistamine for at least 5 days prior to skin test evaluation. All patients underwent a skin testing protocol with PPL, MDM, penicillin G, ampicillin and amoxicillin. Those with negative SPT underwent IDT with 1/100 PPL and full strength penicillin G and ampicillin. If negative, 1/10 PPL is given followed by full strength of PPL. In case of negative PPL evaluation, we test with 1/100 MDM, followed by 1/10 and then full strength MDM. Normal saline was used as control. Test to all components were stopped when a positive test was obtained. All patients were tested for both total IgE and specific IgE antibody to penicillin with RAST system.
All patients signed an informed consent before testing. They were aware of the remote possible risk of an allergic reaction or anaphylaxis from the testing. Both SPT and IDT were assessed 20 minutes after application and the results were considered positive if a wheal and flare reaction larger than the negative control was present during SPT or 3 mm higher than the injected papule in IDT [26].
Patients with both negative RAST and skin testing performed a single-blinded oral DPT with 300 mg of phenoxymethyl penicillin, potassium salt tablet. Challenge was started at 10% of the total dose of the active principle and doses were increased 2 folds every 60 minutes until the total dose was reached. DPT was performed in a ward with full resuscitation support and continuous monitoring by physician and a nurse. The DPT was scheduled at least 6 weeks after suspected drug reaction and 5 days after H1-antihistamines withdrawal. DPT was considered negative if no signs of suspected IgE mediated reaction occurred. Patients who displayed no symptoms remained in hospital for at least 2 hours after the last challenge and maintained a contact with the hospital after discharge to report any delayed drug reaction [27].
RESULTS
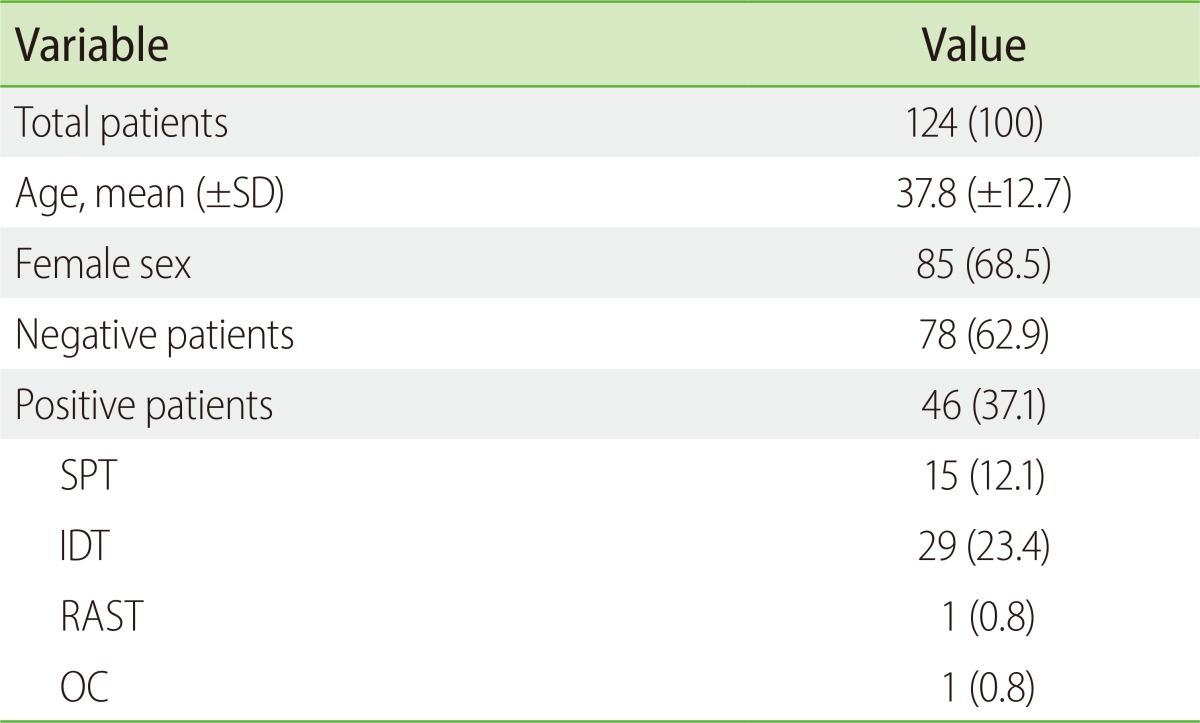
A total of 124 patients underwent a full drug allergy evaluation for penicillin antibiotics. Mean age was 37.8 (standard deviation, 12.7) years, with range from 8 to 74 years. 39 male (31.5%) and 85 female patients (68.5%) were included. Diagnosis of penicillin drug allergy was confirmed in 46 patients (37.1%); of which 14/39 males (35.9%) and 32/85 females (37.6%) (Table 1).
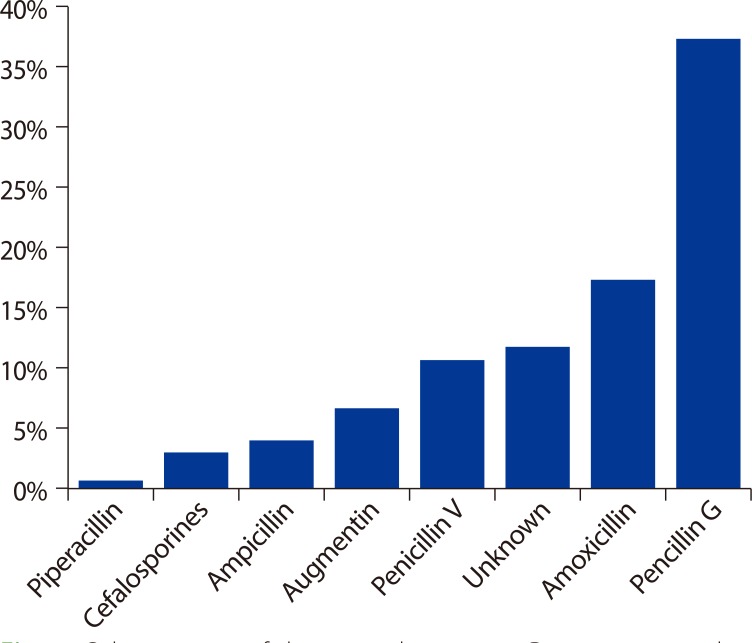
Data of culprit drug was available in 108 patients. The leading culprit drug was penicillin G in 48 patients, followed by amoxicillin in 25 patients, penicillin V in 16, amoxicillin/clavulanic in 9, ampicillin in 5, cephalosporines in 4, and piperacillin in 1. Up to 4 patients reacted to two different betalactams. Culprit drug was not available in 18 patients (Fig. 1).
Among the 44 confirmed positive patients by means of skin testing, we had 15 patients (34.1%) positive by SPT and 29 (65.9%) by IDT. Among the different reagents tested; we had 21 patients (47.7%) positive to PPL, 9 (20.4%) to MDM, 18 (40.9%) to ampicillin, 22 (50.0%) to Penicillin G skin testing and 6 (13.6%) to amoxicillin SPT. One patient had a positive RAST and one patient had a positive DPT with an immediate urticarial reaction (Table 2).
Among patients who had positive tests exclusively to a single component of the testing battery, 7/44 patients (15.9%) were exclusively skin test positive for PPL, 5/44 (11.4%) for MDM, 5/44 (11.4%) for penicillin G, 3/44 (6.8%) for ampicillin, and 2/44 (4.5%) for amoxicillin.
Regarding patients reacting exclusively to a combination of reagents, 12/44 (27.3%) had exclusive response to PPL and/or MDM, 17/44 (38.6%) had exclusive response to penicillin G, amoxicillin or ampicillin and not to PPL and/or MDM, 23/44 patients (52.3%) with exclusive responses to PPL and/or MDM and/or penicillin G, and 17/44 (38.6%) reacted exclusively to PPL and/or penicillin G.
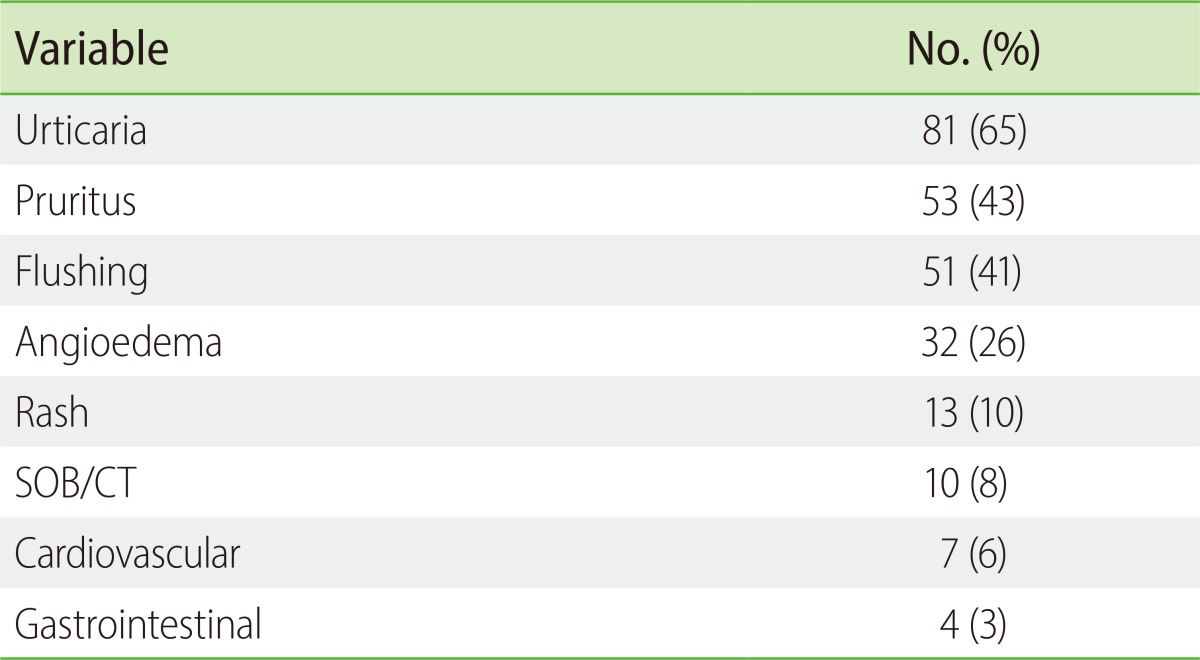
Clinical spectrum of patients presentation included urticaria, pruritus, flushing, angioedema, rash, shortness of breath, hypotension and syncope (Table 3).
Six out of nine patients (66%) tested positive to MDM (SPT or ID) had severe clinical presentation including shortness of breath, angioedema, and hypotension compared to 11/21 of patients (52%) who tested positive to PPL (SPT or ID).
No significant differences were observed in terms of age, and sex for patterns of skin testing. There was no systemic reaction during skin testing.
DISCUSSION
To our knowledge, this is the first descriptive, long studied evaluation looking at the patterns of penicillin hypersensitivity in a gulf country. Unlike previous studies in the gulf area, we performed a full drug allergy evaluation [28].
Similar to other studies [3, 29, 30, 31], we had a predominance of female being evaluated 85/124 (68.5%), with similar rates of confirmed drug hypersensitivity between both sexes and similar age differences.
We report a 12/44 (27.3%) exclusive positive response to PPL and/or MDM, compared to other reports of 14.7% [32], 21.3% [33], 46.9% [34], 47% [35] or 54.7% [36] exclusive responses to PPL and/or MDM. In a study from Romano et al. [33], 78/300 of patients (26.0%) were exclusively positive to PPL and/or MDM and/or Penicillin G compared with 23/44 (52.3%) in our group.
Interestingly, 17/44 of our patients (38.6%) with positive skin test results had positive responses to Penicillin G, Amoxicillin or ampicillin but not to PPL and/or MDM. Other studies showed that patients with positive skin tests to reagents other than PPL or MDM was 26.6% [34] or up to 62.6% [32, 37] in 2 studies from the same group.
About 11.4% of patients had positive response exclusively to penicillin G, which is a higher value compared to other reports [33]. Romano et al. [33] have shown 2.7% exclusive positive skin response to penicillin G. Furthermore, amoxicillin and ampicillin testing was required in our study for diagnosis in up to 4.5% and 6.8% of patients for each reagent respectively, compared with 3.3% and 12.3% respectively, from other studies [33].
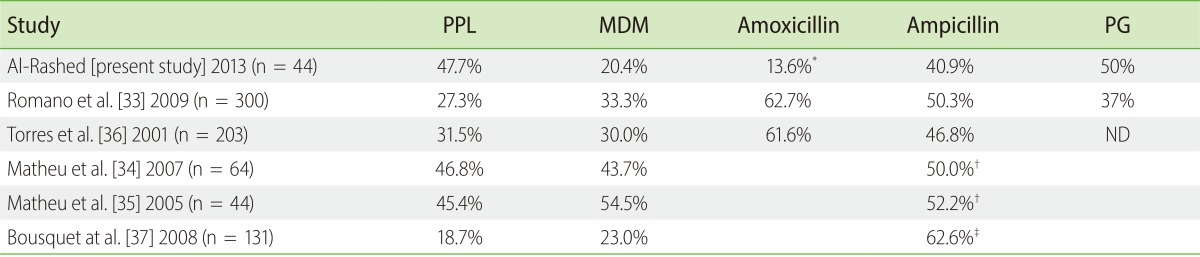
Comparative results of our findings of positive skin tests with other studies are shown in Table 4. We report high rates of positive response to PPL, similar to the findings of Matheu et al. [34, 35]. Despite the reported high rates of PPL positivity, the frequency of positive IDT responses to PPL is most likely underestimated as we started testing with 1/100 of PPL in a first step along with full strength undiluted concentration of Ampicillin (25 mg/mL) and Penicillin G (10,000 U/mL). This might lead to overestimation of positive ampicillin and Penicillin G skin testing. Besides, our findings of low positive IDT to MDM are similar to the data from Bousquet et al. [32] and might be even underestimated because patients who had positive IDT to any other reagent were not tested to MDM in our cohort. Unexpectedly and despite our protocol that overestimates ampicillin and penicillin G positive skin testing results, we observed a slight decrease in the rates of positive results to both reagents compared with other studies [33, 36]. IDT reagents for amoxicillin were not available during the period of study and this can explain the lower rates of positive results to amoxicillin in our cohort. We terminated the tests if patients were tested positive to any SPT or IDT reagents.
Many protocols and published data have shown a variability among reported negative predictive value of skin testing for major determinants, mixture of minor determinants and penicillin G, ranging from nearly 100% [1, 38] to 90-70% [5, 17, 29, 36, 37, 39], with significant regional differences between European and American studies [37, 38]. Our data is more in accordance with American studies reporting 99% negative predictive value [1], although this data must be taken with caution as stated in the limitations section below.
In accordance with other studies, we have not reported any systemic reaction during skin testing. Low rates of systemic reactions have been described [1].
DPT was positive in only one case (2.2%) in our study. Compared with other studies with skin testing to PPL, MDM, Penicillin G, and Amoxicillin, where DPT was needed in 4.3% [35], 7.2% [34], 7.7% [32], 16.9% [36], and 17.2% [31] of patients.
We had 46/124 of patients (37.1%) confirmed as allergic for penicillin. This is relatively high percentage of positivity, and different from the usual reported 10% [1, 2, 5, 6]. However, similar rates of positivity were reported in a study from Turkey (36.2%) [31]. Our confirmed high numbers could be even underestimated as anaphylactic patients were not included. This relatively high percentage of positivity might alarm physicians and general practitioners, and acknowledge the importance of drug allergy history in patients.
RAST and enzyme-linked immunosorbent assay are also used to detect IgE antibodies, but only to the major penicillin determinant and therefore, these tests are less sensitive than the skin test [40]. In our study only one patient (2.2%) was confirmed with penicillin allergy by means of RAST positive specific IgE, compared with other reported rates of in vitro IgE antibodies (6.1-17.8%) [29, 36]. The increased percentage of negative test together with the increased sensitivity of CAP system [40, 41] lead us to stop performing RAST to penicillin in our clinic after this study.
Desensitization is required when betalactam hypersensitivity is confirmed and betalactam treatment is the drug of choice [42]. Oral and intravenous protocols for betalactams desensitization have been published [42, 43, 44, 45, 46] starting from very small doses that are usually doubled every 15 minutes until the full therapeutic dose is achieved. The possible reactions during the procedures are mostly mild in nature, but severe ones are possible [42]. Desensitization is maintained by continuous treatment with the culprit betalactam [47]. In our study, we did not have any case that required desensitization to betalacatm, as patients could use alternative first-line medications.
Several limitations should be acknowledged in this study. First, many of our patients were tested for remote reactions more than 10 years ago, in the absence of drug allergy evaluation service in Kuwait. There is a concern on reported resensitization after allergic tests up to 27.9% [24]. Our patients were not rechallenged [1, 26, 48], although none of the negative patients return to our clinic with a reaction to penicillin. Second, we used phenoxymethyl penicillin 300 mg tablet for DPT. Third, we have not considered the changing patterns of sensitization with the increasing use of amoxicillin and cefalosporins [49]. Patients reporting reactions to penicillin and semisynthetic penicillins were challenged with phenoxymethyl penicillin, so we are missing patients with side-chain sensitization [21, 22, 23]. Last, immediate anaphylactic patients were not included in this study. Torres et al. [36] have studied 290 Spanish patients with positive allergy history for betalactams including anaphylactic patients, skin tests were positive in 70.3% of the cases and DPT was needed in 16.9% patients.
It would have been interesting to evaluate the diagnostic value of in vitro specific IgE determination by the CAP System instead RAST in our Arabian Gulf population. We are also aware on the low number of drug allergy referrals, when compared with other populations [29] and this can be most likely related to the recent availability of drug allergy evaluation service.

 XML Download
XML Download