

 PDF
PDF ePub
ePub Citation
Citation Print
Print


BACKGROUND
The prevalence of allergic diseases has grown in Finland during the last 50 years, similarly to many other industrialized and urbanized countries (Fig. 1). Although the origin of allergy remains unresolved, increasing body of evidence indicates that the modern man living in urban built environment is deprived from environmental protective factors (e.g. soil micro-organisms) that are fundamental for normal tolerance development. Reduced contact of people with natural, biodiverse environments may adversely affect the human commensal microbiota and its immunomodulatory capacity. Recent results from North Karelian teenagers have prompted the so called biodiversity hypothesis, which enlarges the hygiene- and microbial deprivation hypotheses by taking into account the interrelationships of three DNA compartments: human cells, skin-mucosal microbiomes and environmental microbiomes [1-3]. The current dogma of allergen avoidance has not proved effective in halting the 'allergy epidemic', although allergen avoidance is, and will stay, in the treatment armamentarium of individual patients. It is the Finnish consensus that restoring and strengthening tolerance is the key to a better immune balance and should more be in focus. Understanding the mechanisms of tolerance paves also the way from treatment to prevention and better public health.
GOALS
The 10-year implementation programme [4, 5] is aimed to reduce burden of allergies both at the individual and societal levels. The main goals are to: 1) prevent the development of allergic symptoms; 2) increase tolerance against allergens; 3) improve the diagnostic quality; 4) decrease work-related allergies; 5) allocate resources to manage and prevent asthma and allergy attacks; 6) decrease costs due to allergic diseases. The goals are also numeric, e.g. asthma emergency visits should drop 40% in 10 years. The key messages for health-care, decision makers and general public are given in Fig. 2.
METHODS
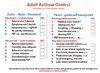
For each goal, specific tasks, tools and evaluation methods are defined. As an example of recent tools, practical recommendations for the childhood allergies were published in March 2012 [6, 7]. Mild allergic symptoms are very common and should not be medicalised unnecessarily. Mild allergy is not predestinated to become more severe along time. The outcome is generally favourable [8]. Severe forms of allergy are in special focus. To help patients proactively to stop attacks and exacerbations of severe allergies, simple self-management plans have been launched for 1) allergic rhinitis, 2) anaphylaxis, 3) asthma, 4) asthma in small children, 5) atopic eczema, 6) food allergy, and 7) urticaria. The patients are trained for guided self-management, and disease control is strongly emphasized and educated both to health care personnel and patients (Fig. 3). The allergic inflammation is treated effectively from the very beginning (hitting early and hitting hard) also in other conditions than asthma, like in atopic dermatitis [9]. Importance of patient follow-up and long-term maintenance therapy is stressed. For children with mild persistent asthma (the majority!), a strategy of intermittent (periodic) treatment has been developed [10]. Immunotherapy and especially sublingual immunotherapy (SLIT) is advocated where feasible. Food allergy diets are critically re-evaluated and stopped if possible. Specific oral tolerance induction (SOTI) for milk, wheat and peanut has been studied intensively and employed increasingly in clinical practice [11]. Long avoidance lists of allergens or irritants have been dropped. Avoidance must be based on proper diagnostic work and must be precise: what is avoided and how long? In patients with troublesome food allergies, a clear shift from passive avoidance to active treatment has been taken.
Nationwide implementation acts through the network of local public health coordinators (GPs, nurses, pharmacists). In addition, three non-governmental organisations (NGOs) have started 2011 a 4-year project to implement the new recommendations among allergic people and general public. The 21 central hospital districts are carrying out a three-step educational process: 1) two hour programme launch sessions for opinion leaders, coordinators, and educators of NGOs, 2) educational sessions in large health centres, 3) one day courses in central hospitals for local health care personnel. In years 2008-2012 Finnish Lung Health Association (Filha) has organized 150 educational events with more than 9,000 participants (25% physicians, 50% nurses, 10% pharmacists, 15% others). The main themes have been: allergy-healthy child, anaphylaxis, food allergy, improving tolerance, and asthma. Eleven allergy testing centres have been audited for good diagnostic practice and given a certificate.
OUTCOMES
For outcome evaluation, repeated surveys are performed and health care registers employed at the beginning, at 5 years, and at the end of the programme. The messages of the programme have been well received by health care personnel [12], and attitudes are changing. For example, GPs scored the message of improving tolerance 9.1 in a scale 4-10. In an internet-based gallup survey, allergic people gave the best score to the message "Support health, not allergy" and only 12% agreed with the claim "Avoidance is the best strategy to combat allergy" [13]. Emergency visits and hospital days caused by asthma are in steady decline (54% during the last 10 years), but to reduce them further needs risk group thinking [14]. The small children and especially women 60 years or older should be in focus. Anaphylaxis emergency visits have even increased, which may have resulted from improved education and awareness. The differences in asthma and anaphylaxis visits are large between different regions of the country, which probably tells more of the variable health care practices than of true differences in occurrence [15]. Asthma seems to become a milder disease, or better controlled, according to a pharmacy barometer survey: 10% of asthmatics evaluated their disease as severe in 2001, while the corresponding figure was 4% in 2010 (manuscript in preparation). In terms of disease prevalence and incidence, data is not yet available of the long-term follow-up studies.
CONCLUSION
The Finnish initiative is a comprehensive plan to change the course of allergy in the society. This is done by increasing both immunological and psychological tolerance (Fig. 4) and changing attitudes to support health, not allergy. Early and effective treatment of severe allergies is strongly emphasized. Guided self-management is the key to stop attacks proactively. The preliminary results are promising. Several health care indicators are showing that the allergy burden is levelling off in Finland and even decreasing.
The Finnish Programme, or parts of it, is associated with the World Allergy Organization (WAO) [16], Global Initiative for Asthma (GINA) [17], and WHO/GARD (Global Alliance against Chronic Respiratory Diseases). The Programme is developed further and enlarged along with an EU-funded project, MeDALL (Mechanisms of the Development of Allergy) [18]. A Norwegian Allergy Programme is under construction, and with the Finnish one, will give a model for others to modify and improve to meet their special needs.
It is time to re-evaluate the allergy paradigm and implement new kind of actions, when allergic individuals are becoming a majority of Western populations and their numbers are increasing worldwide [16]. National and local action plans, with clear targets, are needed to meet the challenge. They do work [19]. Allergy is a community problem needing community actions. An interesting example is the Korean initiative, where multi-sector cooperation is taking place (government, academic institutions, private organizations, local communities, media) to tackle the allergy burden [20, 21].


 XML Download
XML Download